

Constant rate infusions (CRIs) have become more commonly used in veterinary practice over the past decade. A CRI refers to a drug being injected at a specified dose over a continuous period, usually by the intravenous route. Technically, where a drug is administered continuously but with changes being made to the dose, it is termed as a variable rate infusion (VRI), however the term CRI is usually applied to both situations. When CRIs are used to reduce inhalational anaesthetic agent requirement, it is known as partial intravenous anaesthesia (PIVA). Where a CRI is used alone to provide anaesthesia, it is termed total intravenous anaesthesia (TIVA) (Duke, 2013).
CRIs of many drugs provide balanced anaesthesia protocols as they provide varying amounts of analgesia, narcosis and muscle relaxation, allowing reduced reliance on inhalational agents. This reduced reliance on inhalation agents is beneficial as CRI agents generally cause less depression of cardio-respiratory systems than traditional inhalation agents, and using different agents in a multi-modal combination again reduces negative side effects. CRIs may also be continued into the recovery phase benefitting the patients with a smoother and more comfortable recovery. They also allow for careful titration of dosage and weaning (Duke, 2013).
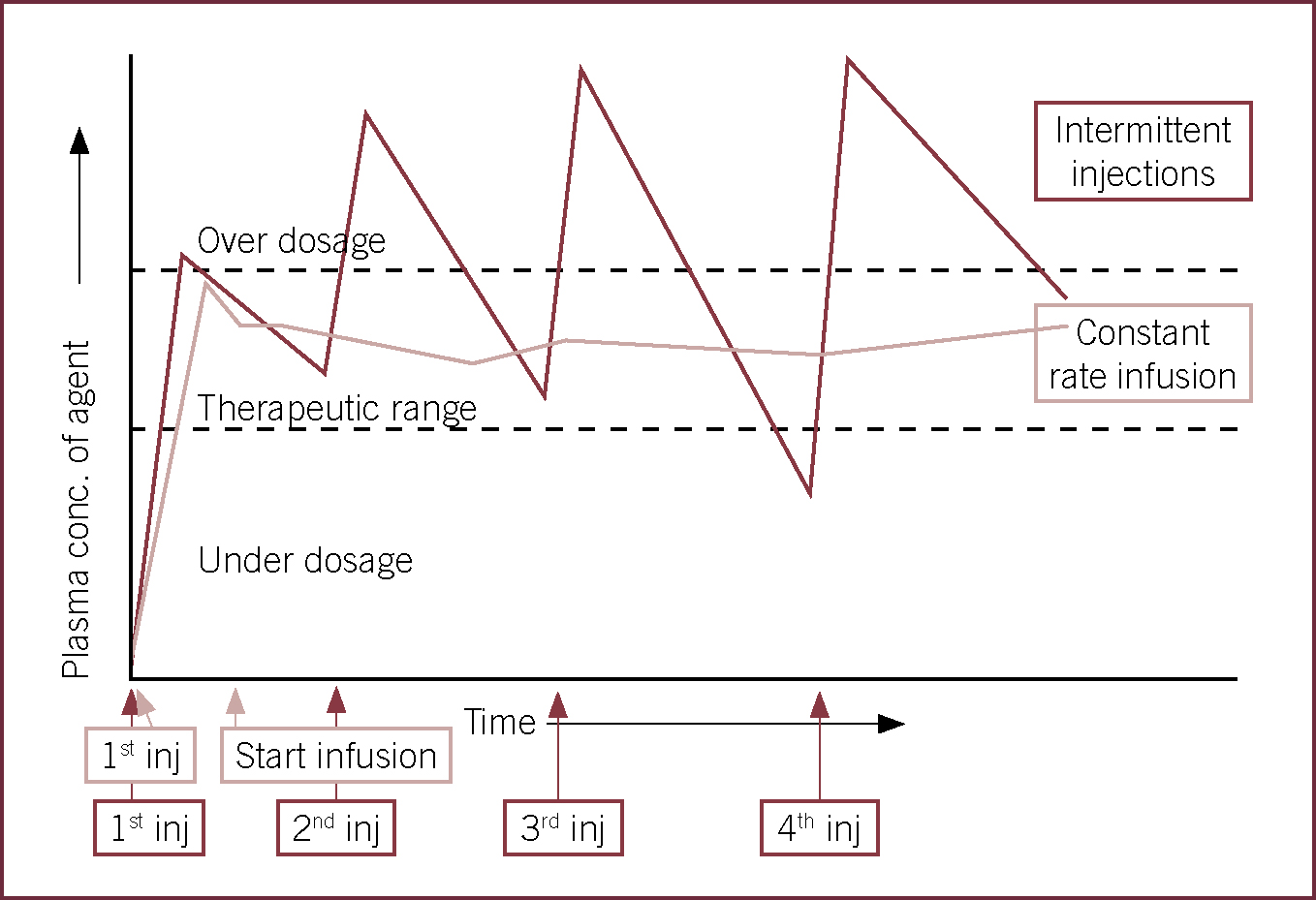
Pharmacokinetically, the benefit of CRIs over intermittent boluses is that the former maintains drug action at receptor sites by maintaining plasma concentration whereas plasma concentrations continuously drop after a peak level has been achieved by the latter. Repetition of drug boluses can result in a ‘saw-tooth’ effect of drug action and mistimed boluses can result in either under or overdosing of the drug (Figure 1).
For a CRI to maintain plasma concentrations, the infusion rate needs to equilibrate with drug clearance. Plasma concentration is affected by distribution, redistribution, metabolism and excretion; these factors influence the rate of delivery and in combination with the offset times of the drug, the duration of infusion to prevent drug accumulation. Often, if an infusion is started at the set infusion rate, drug onset time will be prolonged as drug clearance will commence before adequate plasma levels are reached; therefore, most drugs require a bolus (loading dose) to be given at the beginning of the infusion (Hill, 2004).
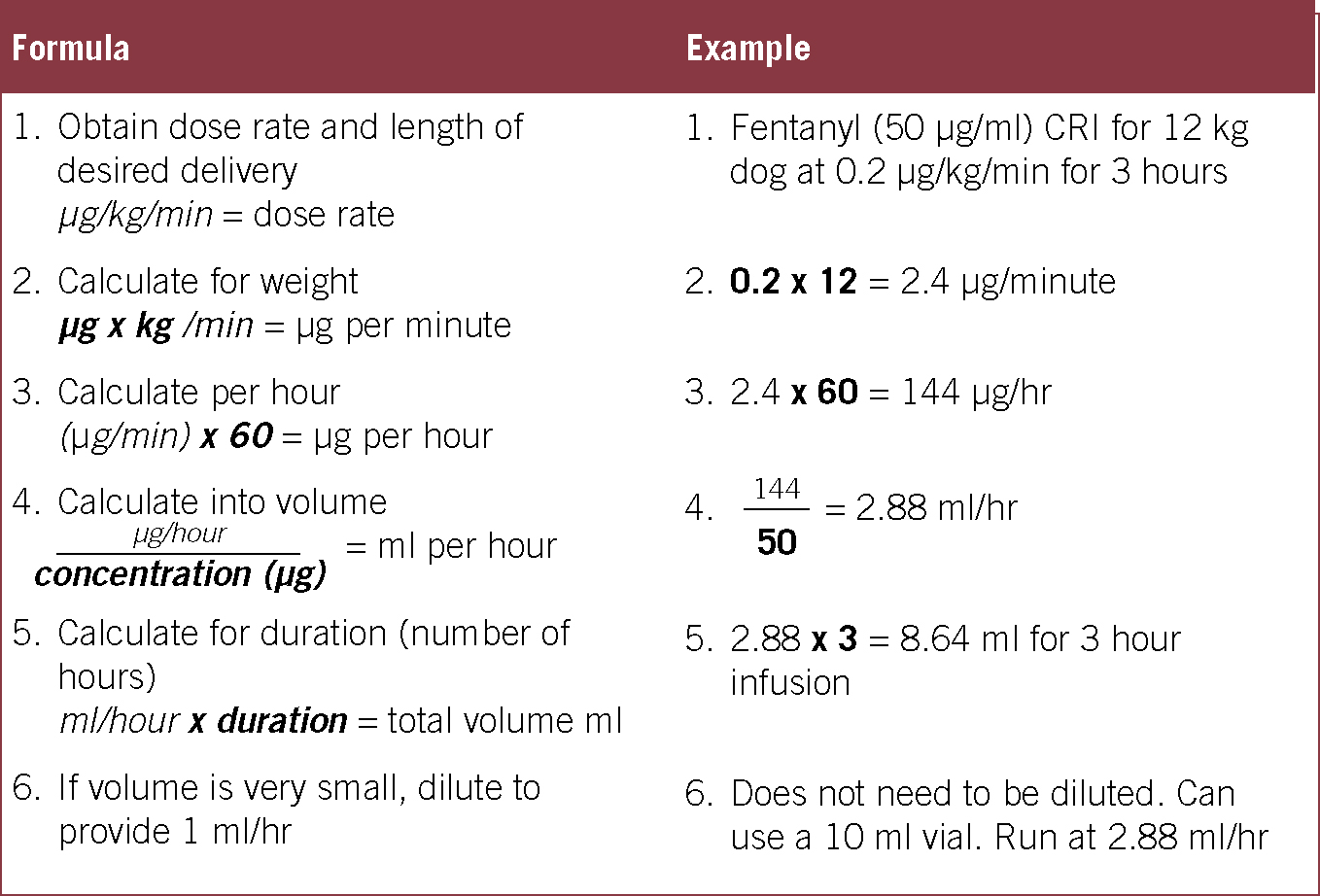
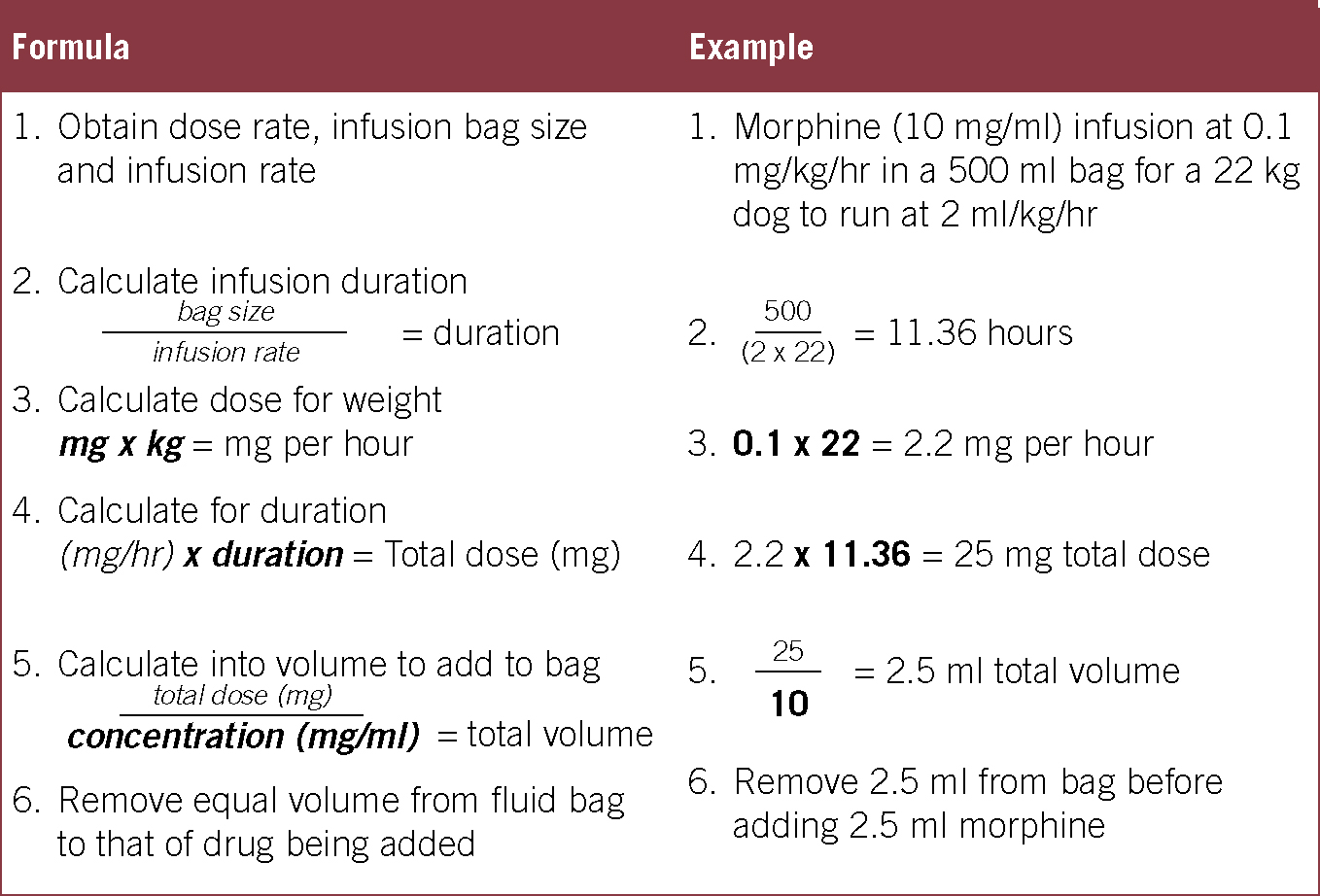
Accurate CRIs require the use of a syringe driver or a precise fluid pump. Equipment should be serviced in accordance with the manufacturer's recommendations to ensure it is correctly calibrated. The correct consumables should be used with said equipment as this also will affect the calibration; many syringe drivers provide a choice of standard brand syringes. Table 1 compares the advantages and disadvantages of CRIs. Practical tips for CRIs can be found in Table 2 and a guide to calculating CRI rates in Figures 2 and 3.
Table 1. Advantages and disadvantages of constant rate infusions
| Advantages | Disadvantages |
|---|---|
| Steady plasma levels of drug | Lengthy set up |
| Safer (avoids intermittent overdose) | Equipment required |
| Reduced dosages and therefore side effects | Risk of long-term overdose if calculations are incorrect |
| Easier over long term | Reduced patient contact: risk of reduced intravenous care |
| Reduced patient contact; allows patient more rest time | Hospital stay required |
| Easy to adjust levels | |
| Reduced consumable costs (multiple syringes/needles/vials used for intermittent dosing) |
Table 2. Practical tips for constant rate infusions (CRIs)
| Use syringe drivers for more accurate, shorter duration infusions |
| Use fluid pumps for longer infusions where drugs are highly diluted |
| All drugs mentioned can be diluted in compound sodium lactate or saline |
| Dilute drugs depending on patient size to provide workable volumes. Diluting to 1 ml/hr or 1 ml/kg/hr is recommended for easy titration |
| Practice calculations to feel confident working them out in a hurry; drug calculators are also useful when you are in a rush — look on the internet or design your own using Excel |
| Have dose ranges calculated, written down and kept to hand |
| Inhalational agents can be slowly reduced once the loading dose is active. For fast acting drugs like Fentanyl this can be almost immediately |
| Consider lowering dosages or stopping infusions before patient recovery to prevent dysphoria |
| Label syringes and fluid lines with drug's name to prevent confusion; take care not to accidently flush through a line of concentrated drug |
| Attach CRIs as close to the patient as possible; use needle free valves and Y-connectors where possible |
Morphine
Morphine is a mu-agonist opioid and accordingly provides analgesia suitable for moderate-severe pain. CRIs of morphine have been used and studied widely. Morphine CRIs achieve steady levels of analgesia at lower dosages than intermittent boluses and have minimal side effects even in critical patients. Morphine CRI has been shown to reduce minimum alveolar concentration (MAC) of isoflurane in dogs by 48% (Muir et al, 2003) and is normally well tolerated in recovering and conscious patients, although cats are more likely to show dysphoria than dogs (Bromley, 2012). Nausea is less commonly linked to morphine CRIs than morphine boluses.
Methadone
Methadone is the only licensed full mu-agonist opioid, although it is unlicensed for CRIs (as is morphine). Methadone CRIs are used in veterinary medicine, although there are minimal published data. Methadone causes less nausea than morphine which may be beneficial and also has action at the N-methyl-D-aspartate (NMDA) receptors, which may be beneficial for patients suffering from chronic pain (Monteiro, 2009).
Fentanyl
Fentanyl is a lipid bound mu-agonist opioid (Figure 4). It is a faster acting, shorter duration and more potent opioid than morphine and methadone. It is indicated to treat severe pain, but has excellent anaesthetic agent sparing effects so can be used for surgical procedures on critical patients to reduce requirements of vasodilating inhalation agents (Steagall, 2006). It causes dose-dependent respiratory depression and bradycardia and so it is suggested to begin infusions at the lower end of the dose range and increase as required. The use of ventilators and anticholinergics can successfully be used to offset side effects. Relatives of fentanyl include remifentanyl, alfentanyl and sufentanil; these agents are faster acting again than fentanyl and can be useful in cases where rapid metabolism is required (Duke, 2013).

Lidocaine
Lidocaine is widely used for its local anaesthetic and antiarrhythmic properties, but when used systemically also provides analgesia, has a MAC sparing effect (Figure 5) (Matsubara et al, 2009), and has antiinflammatory and free radical scavenging properties (Cassuto et al, 2006). It has minimal negative side effects, although care needs to be taken not to reach toxic doses: for this reason it is generally avoided in cats. It can be useful in septic and gastro-intestinal cases as it may reduce the risk of disseminated intravascular coagulation (DIC) and systemic inflammatory response syndrome (SIRS) (Cassutto et al, 2003). Lidocaine can be beneficial in providing balanced analgesia with opioids and ketamine.

Ketamine
Ketamine is a dissociative anaesthetic agent that is used for induction of anaesthesia or sedation in people, horses, dogs and cats. Its side effects including dysphoria, muscle rigidity, mydriasis, and increased sympathetic drive are well known. Ketamine also has analgesic effects and is inhalation anaesthetic agent sparing; these effects are appreciated at much lower dosages than generally used for anaesthesia, reducing many of its negative effects. Ketamine acts as an antagonist on the NMDA receptors which are located in the dorsal horn of the spinal cord and the brain. These receptors are involved in heightening the pain sensations of continuous noxious stimulus, which can lead to central sensitisation and its associated symptoms of allodynia and hyperalgesia. By reversing the activation of the NMDA receptors, ketamine is particularly useful for patients suffering from chronic pain.
A bolus of ketamine can provide analgesia for up to 20 minutes, but a CRI can be used for several days. Low infusion rates (analgesic dosages) can provide around 25% reduction of MAC of isoflurane in dogs (Muir, 2003). Side effects at analgesic dosages are minimal but can include increased heart rate, increased systolic blood pressure, sporadic breathing and dysphoria in the conscious patient. Titration of infusion rate will often suitably reduce or subdue side effects (Duke, 2013). Ketamine should be used to provide balanced analgesia along with opioids, and its use is commonly regarded as contraindicated in patients at risk of raised intraocular or intracranial pressure. Ketamine is widely used in human disaster and emergency medicine due to its positive effects on sympathetic drive, although it can be detrimental in end-stage shock (Jolly et al, 2007).
Medetomidine/dexmedetomidine
Medetomidine and dexmedetomidine are alpha-2 adrenergic agonists that are commonly known for their sedative effects. They are potently MAC reducing, and even low dose CRIs have been shown to markedly reduce MAC of isoflurane. Alpha-2 agents cause peripheral vasoconstriction which often triggers a reflex bradycardia, however they are generally associated with maintaining acceptable mean blood pressure; nevertheless their use is generally reserved for haemodynamically stable patients. Other side effects include increased urine output and hyperglycaemia (Duke, 2013).
Alpha-2 agonists also provide analgesia: in horses visceral analgesia from alpha-2 agents can be as potent as opioid analgesia (Muir, 1985). In dogs and cats alpha-2 agonists are generally used alongside other analgesics (namely opioids) to provide superior analgesia as the agents work synergistically. Alpha-2 CRIs can be used on conscious patients to provide titratable sedation during recovery (Bromley, 2012).
Analgesic combinations
Morphine, lidocaine and ketamine is the most commonly used combination of agents. One combination has been shown to reduce MAC of isoflurane by 45% in dogs (Muir, 2003). Morphine plus ketamine infusions are commonly used in cats to avoid lidocaine toxicity. Other analgesic agents mentioned work synergistically and there are no published contraindications to co-administering them. Combinations of drugs should be tailored to ensure provision of suitable multimodal analgesia while avoiding unnecessary polypharmacy. Combining drugs in one solution compared to multiple separate infusions should also be considered; advantages of the former include ease of administration, while the advantage of the latter is greater titration options.
Midazolam
Midazolam is a benzodiazepine which provides sedation, muscle relaxation, and amnesia with minimal cardiovascular side effects. Its use in healthy animals can cause excitation if administered alone, thus its use is reserved for sicker patients, or in combination with other sedatives. It can be administered as a CRI to provide greater centrally mediated muscle relaxation, however this has no known analgesia effects. The antagonist flumazenil is available and may be required after long infusions (Duke, 2013).
Propofol
Propofol is an alkylphenol anaesthetic agent that is commonly used for induction of anaesthesia as it is associated with rapid smooth inductions. Its use as a TIVA agent is well reported, causing mild, but tolerable, cardio-depressant effects but often significant respiratory-depressant effects that may require ventilatory support (Suarez 2012). It is reportedly used in PIVA protocols to reduce vasodilatory effects of volatile agents. Sub-anaesthetic CRIs are also reported in intensive care settings (Duke, 2013).
Anaesthetic depth monitoring of patients receiving a propofol TIVA is comparable to that of volatile agents, and a VRI can be instituted to rapidly change anaesthetic depth. Effects from propofol TIVA can become cumulative in cats as it is less effectively metabolised, so long infusions need to be titrated downwards to prevent prolonged recoveries. Otherwise recovery from propofol TIVA is generally smooth and rapid (Duke, 2013).
Alfaxalone
Alfaxalone is a neurosteriod used for smooth rapid induction of anaesthesia, and TIVA. Similarly to propofol, a VRI can be used to rapidly change anaesthetic depth and monitoring is comparable to that of an anaesthetic maintained by volatile agent. Again, as with propofol, alfaxalone causes some cardiovascular depressant effects and can cause hypoventilation when used for TIVA (Suarez, 2012). Alfaxalone is non cumulative, and while recovery times are generally acceptably quick, they may be slightly longer then recoveries from propofol TIVA (Suarez, 2012).
Dosages for each drug can be found in Table 3.
Table 3. Dosages for PIVA and TIVA drugs
| Drug | Loading dose | Dose rate/kg/minute | Dose rate/kg/hr | Clinical cases where may be of particular use |
|---|---|---|---|---|
| Morphine/methadone | 0.1–0.3 mg/kg (this can be given as premedication) | 1–3 μg | 0.1–0.2 mg | Moderate to severe pain MAC reducing |
| Fentanyl | 3–5 μg/kg | 0.1–0.6 μg | 6–36 μg | Severe painHigh risk patients |
| Ketamine | 0.5–1 mg/kg | 10–20 μg | 0.6–1.2 mg | Chronic PainSomatic pain |
| Lidocaine (dog) | 1–2 mg/kg | 20–100 μg | 1.2–6 mg | GI surgery, sepsis, splenectomy |
| Dexmedetomidine | 0.5–1 μg/kg | 0.008–0.015 μg | 0.5–1 μg | Complex pain, bouncy dogs |
| Medetomidine | 1–2 μg/kg | 0.004–0.03 μg | 1–2 μg | Complex pain, bouncy dogs |
| Midazolam | 0.2–0.4 mg/kg | 0.3–0.8 μg | 0.02–0.05 mg | Pelvic surgery |
| Propofol | 4–6 mg/kg | 0.2–0.5 μg | 12–30 mg | Avoidance of inhalational anaesthesia |
| Alfaxalone | 1–2 mg/kg | 0.06–0.15 μg | 4–9 mg | Avoidance of inhalational anaesthesia |
PIVA, partial intravenous anaesthesia; TIVA, total intravenous anaesthesia
Vasopressor and inotropic agents
The following drugs are all classed as ‘catecholamines’ and all act on the sympathetic nervous system; they are used clinically for treating hypotension. Their actions are all to increase blood pressure but in different ways: ‘vasopressors’ constrict blood vessels; ‘chronotropes’ increase heart rate, and ‘positive inotropes’ increase cardiac contractility. They are suited as CRI agents as they are rapid acting, not requiring a loading dose, but short lasting.
Dopamine
Dopamine is the natural precursor of norepinephrine and epinephrine and has several dose-dependent effects (Hollenberg, 2009). At very low doses it acts on dopaminergic receptors and causes vasodilation at renal and mesenteric capillary beds, which may have renal and gut protective benefits. Clinically, however, it is usually used at higher doses where it has actions initially at beta-1 receptors producing positive inotrope and chronotrophic actions and secondly at alpha-1 receptors producing vasopressor actions. CRI doses can be increased until suitable mean arterial blood pressure is reached. Its effect is minimised where acepromazine has been given although it is still clinically useful (Monteiro, 2007).
Dobutamine
Dobutamine predominantly affects beta receptors and so reliably produces inotropic and then chronotropic actions. Its use for treating hypotension under anaesthesia is minimal as most anaesthetised patients will be suffering from vasodilation (Dyson, 2006). It can still be a useful treatment for hypotension where cardiac filling pressures are deemed adequate.
Phenylephrine
Phenylephrine is a selective agonist at the alpha-1 receptors. This causes reliable vasoconstriction, without any direct cardiac effects. It is mainly of use in septic patients where hypotension is a result of vasodilation, but patients are suffering from, or at risk of tachyarrhythmias from inotropic or chronotropic agents (Hollenberg, 2009). Phenylephrine will cause vasoconstriction of the coronary vessels that may be significant in patients with heart disease. Reflex bradycardia is also a possibility as blood pressure rises. Phenylephrine is recommended to be given by a central vein in human medicine due to the risk necrosis following accidental tissue infiltration (Cooper, 2008). Phenylephrine does require a loading dose.
Noradrenaline
Noradrenaline is a potent alpha-1 agonist, with some agonist action at beta receptors. Therefore it causes reliable vasoconstriction, with some increase of heart rate and stroke volume. It is more potent than dopamine and is often used as a second line drug following dopamine therapy. It is particularly of use in septic patients. Renal damage is risked in hypovolaemic patients, so adequate fluid therapy is paramount (Hollenberg, 2009).
Patients receiving catecholamine CRIs should be weaned off slowly, with continued blood pressure monitoring. A summary of drugs and dosages can be found in Table 4.
Table 4. Summary and dosages for catecholamine treatment
| Drug | Receptor action | Effects | Dosages |
|---|---|---|---|
| Dopamine | Beta-1Alpha-1 | Vasodilation of renal and mesenteric arteriesInotropicVasopressor | 2–20 μg/kg/min |
| Dobutamine | Beta-1Beta-2 | InotropicChronotropic | 2–10 μg/kg/min |
| Phenylephrine | Alpha-1 | Vasopressor | Loading dose: 2–5 μg/kgInfusion: 0.1-1.0 μg/kg/min |
| Noradrenaline | Alpha-1Beta-1Beta-2 | VasopressorSome chronotropic and inotropic effects | 0.01–0.05 μg/kg/min |
Conclusion
Intravenous CRIs are a valuable tool during anaesthesia. Using CRIs to provide the analgesic, narcotic and muscle relaxing components of a balanced anaesthetic protocol reduces the dependence on vasodilating agents such as isoflurane. This opens their use for not only painful patients but also patients at high risk of hypotension from ‘standard’ anaesthetic protocols. Hypotension is a frequent complication in veterinary anaesthesia and although drug therapy should not be a primary treatment, it does provide a valuable solution. CRIs should be practiced by veterinary professionals with knowledge of the techniques and drugs, and access to the correct equipment to administer them.
Key points
- Constant rate infusions (CRIs) provide stable plasma concentrations of drugs, preventing peaks and troughs of drug action.
- Analgesic, narcotic and muscle relaxant agents can be provided by CRI to minimise reliance on inhalation anaesthetics, reducing vasodilatory effects.
- Treatment of hypotension with drug therapy generally requires CRIs. Several drug