
When a patient is identified that is experiencing cardiopulmonary arrest (CPA) veterinary professionals need to act quickly in order to promote a positive outcome. Preparedness, team training, having an organised, stocked crash trolley, administering chest compressions and ventilating the patient are all key parts to basic life support (BLS). There are several other interventions that can also be considered once BLS has started which may help to achieve return of spontaneous circulation (ROSC). Recommendations for advanced life support (ALS) measures have been published in the RECOVER guidelines in The Journal of Emergency and Critical Care 22(S1): S102–S131 (Fletcher D et al, 2012).
ALS
Access for drug administration
If the patient was already in the hospital there may already be intravenous (IV) access. If not, IV access should be gained promptly. Emergency drugs reach the heart quicker and in more concentrated volumes if given via a central vein but placing a jugular catheter may be technically challenging in a CPA situation. If administering drugs via a peripheral IV catheter, it is recommended to follow the dose with large volumes of saline flush, e.g. 10–20 mls, to ensure they reach the central circulation.
If venous access is proving difficult then there are two other options:
Intra-cardiac administration of drugs is no longer recommended due to the risks associated, such as trauma to the myocardium, laceration to the major vessels and ventricular fibrillation.
Emergency drugs
Only 25 to 30% of a normal cardiac output will be achieved despite even the best technique of chest compressions (Rozanski et al, 2012). The aim of drug therapy is to alter vascular resistance and direct blood flow to the central circulation to protect vital organs. Commonly used emergency drugs (adrenaline and atropine (Figure 1)) dose and mode of action can be viewed in Table 1.

| Drug | Mode of action | Dose | Comment |
|---|---|---|---|
| Adrenaline (epinephrine) Low dose | Drug of choice α and β adrenergic activity — vasoconstriction to improve myocardial and cerebral perfusion pressures |
0.01 mg/kg IV/IO |
Administer every 3–5 minutes |
| Adrenaline High dose | 0.1 mg/kg IV/IO/IT | Start with low dose. |
|
| Atropine | Anti–cholinergic activity |
0.04 mg/kg IV/IO |
Administer every 3–5 minutes |
| Vasopressin | Nonadrenergic peripheral vasoconstrictor — increases myocardial and cerebral perfusion pressures | 0.8 U/kg IV/IO |
Alternate administrations with adrenaline |
IV, intravenous; IO, intraosseous; IT, intra-tracheal
Other drugs
Other drugs may be administered:
Capnography
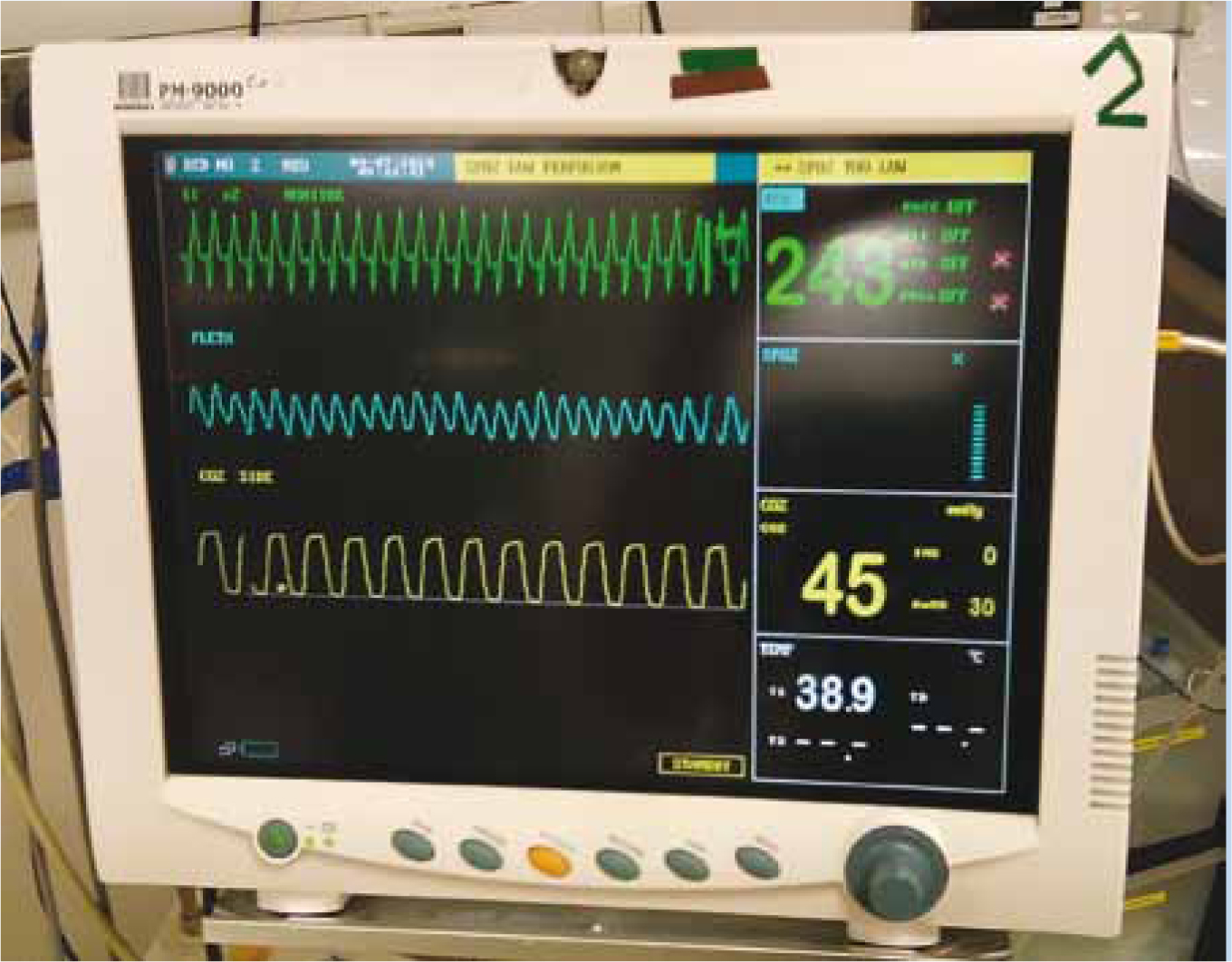
Rozanski et al (2012) recommend end tidal carbon dioxide (EtCO2) monitoring as the best predictor of ROSC and measure for the efficacy of chest compressions (Figure 2). ET tube placement can also be confirmed via a capnograph waveform. Capnograph waveforms represent the amount of CO2 in the air being exhaled. In a normal patient there should be no CO2 detected during inhalation and then there should be an increase in CO2 during exhalation. In a patient experiencing CPA there will be no spontaneous breathing and therefore no CO2 detected. With adequate ventilation and chest compressions low CO2 numbers should be generated on the capnograph. This information can be used to help guide CPR efforts by maximising chest compressions. Once ROSC is established, a dramatic increase in EtCO2 should be observed due to improved circulation. It is agreed that values >15 mmHg in dogs and >20 mmHg in cats are indicative of ROSC (Fletcher et al, 2012).
ECG
There are three arrhythmias that are commonly seen during CPR: asystole, pulseless electrical activity (PEA), and ventricular fibrillation (VF). An ECG should be attached to the patient during CPR so that any arrhythmias can be identified (Figure 3). The ECG trace should be observed every 2 minutes when there is a change in persons administering chest compressions. It is not likely to provide a discernible trace during chest compressions due to the movement of the patient. Although VF is a common arrest rhythm in humans, it is much less common in animals; however, if VF is observed then the treatment of choice is defibrillation.

Defibrillation
Defibrillators may be available in large veterinary hospital settings but are not a common piece of equipment. There are two types available: monophasic (the electrical current flows in one direction); or biphasic (the current flows in one direction and then reverses). Biphasic defibrillators have proved to be superior in terminating VF in humans (Brainard et al, 2012). If VF is identified, hair should be clipped on each side of the thorax (without interrupting chest compressions), liberal amounts of contact gel applied to the paddles and the electrodes should be placed on either side of the thorax over the heart. A dose of 2–4 J/kg should be selected and paddles charged. All personnel should stand back from the table and the operator should shout ‘clear’ before shocking the patient. The ECG should be reassessed for signs of an improved rhythm following defibrillation attempts. The above process can be repeated if VF is still present. Care must be taken if surgical spirit has been used on the patient due to the risk of a fire hazard. A precordial thump can be performed by firmly striking the patient over the heart area with the heel of the hand if the veterinary practice does not own a defibrillator.
Open chest CPR
Cardiac massage via open chest CPR is more effective at generating blood flow than closed chest CPR. The reality is open chest CPR is rarely carried out due to the requirement of significant resources, a highly skilled veterinary team and the requirement for intensive care post CPA. It is recommended that open chest CPR is considered if there is known pulmonary disease such as a tension pneumothorax, or a pericardial effusion (Fletcher et al, 2012).
Monitoring and post cardiac arrest care
Despite initial ROSC in up to 45% of animals, many will re-arrest and die or be euthanased (McIntyre et al, 2014). It is imperative that post cardiac arrest care is optimised as it may positively impact on outcome. Many patients will have developed CPA due to an underlying disease process (such as trauma or sepsis), so every effort should be made to treat this process. Oxygenation and ventilation should continue to be monitored by assessment of mucous membranes, respiration rate and effort, pulse oximetry and capnography. The aim should be to normalise blood oxygenation. There is no need to deliver oxygen therapy if the patient is able to achieve normal oxygen saturation on room air. This can be measured via pulse oximetry or arterial blood gas sampling. Permissive hypercapnia is not recommended and intermittent positive pressure ventilation (IPPV) should be continued until the patient is able to maintain a normal ETCO2. Cardiovascular parameters should be monitored by feeling peripheral pulse quality, blood pressure measurement and continuous ECG monitoring. Hypovolaemia should be managed with appropriate fluids +/- vasopressors.
Mild therapeutic hypothermia (MTH) (32–34°C) is thought to have organ protective effects and lead to improved cardiac and neurological outcomes in humans post CPR (Smarick et al, 2012). It has been suggested that MTH for 24–48 hours may be beneficial to patients that remain comatose post CPR efforts. This intervention would require advanced intensive care and mechanical ventilation so it is not practiced widely, but if patients become mildly hypothermic during CPR it is not recommended to actively warm them. Neurological status should be checked at an appropriate time but may take hours, days or weeks to return to normal. Seizures as a result of cerebral oedema can be managed with diazepam and mannitol.
Basic blood work should be carried out including packed cell volume (PCV) and total protein, and blood glucose electrolytes and acid base should be checked if an analyser is available. Abnormalities should be addressed as discussed previously. If client communication has not yet been made, a team member needs to inform the owners of their pet's current situation and decide on an appropriate plan. It may be helpful to prepare an injectable anaesthetic agent to keep the patient asleep and intubated if time is required to make a decision (e.g. a CPA due to respiratory failure and the owners need to make a decision about euthanasia). The crash trolley should be restocked at this time in case of a re-arrest.
Debriefing
Debriefing should be used as a practical tool to help improve performance and therefore result in improved outcomes. It should be done immediately after the crash so team members can critique the ‘chain of events’ and comment on what went well and areas where further training or clarity are required. This is a free, simple and effective tool which is often neglected and should be seen as equally important as the refresher CPR training sessions.
Consent and ethics
Decisions relating to CPR are often very complicated and multifactorial including disease process, prognosis, cost and emotional factors. For patients with an end-stage incurable disease, the emphasis should be placed on palliative care. Ideally resuscitation status should be discussed on admission with the owners of any critically ill patient in the veterinary hospital. Owner autonomy should be respected and the patient code should be clearly labelled on the hospital sheet as per R — resuscitation, or DNR — do not resuscitate. In the absence of a resuscitation status then CPR should be initiated without a veterinarian's direct order under the theory of ‘implied consent’. The patient's owner should be contacted at the earliest opportunity so the code can be established. It is the veterinarian who is responsible for making the decision to terminate CPR efforts where there is no ROSC.
Conclusion
Despite best efforts to deliver CPR, most resuscitations fail. The success is dependent on many differing factors but there is increasing awareness of the different aspects that can influence a positive outcome. The focus needs to be on ensuring that the team are prepared, trained and that there is effective communication during these high pressured situations to promote a successful outcome.
Key Points
Conflict of interest: none.