Mechanical ventilators are an integral part of any intensive care unit. There are a variety of patients that may benefit from mechanical ventilation such as patients that are hypoxaemic (Pa02 <60mmHg) in spite of oxygen therapy, hypercapnic (PaC02>60mmHg) or at risk of impending respiratory failure. Mechanical ventilation is expensive and requires a dedicated nurse to care for the patient. This nurse must have an understanding of respiratory physiology, principles of mechanical ventilation, terminology, setting up the ventilator, troubleshooting problems, providing nursing care to meet the individual patient requirements and recognising signs of complications. Such cases require thorough clinical records and communication between staff members. They are labour intensive cases but can be extremely rewarding to nurse.
There are a variety of circumstances in which a decision may be made to ventilate a patient. These reasons generally fall into four categories (Clare and Hopper, 2005a).
Hypoxaemia is defined as a PaO2 (partial pressure of oxygen in arterial blood) <80 mmHg. A PaO2 of <60 mmHg indicates severe hypoxaemia and the necessity to act immediately. The most common causes of hypoxaemia are hypoventilation, severe ventilation perfusion mismatch and more rarely diffusion impairment.
Hypercapnia is defined as a PaO2 >60 mmHg. Elevated partial pressure of carbon dioxide in arterial blood (PaCO2) causes respiratory acidosis which may lead to acidaemia, an increased level of hydrogen ions within the blood. The most common cause of hypercapnia is hypoventilation.
Impending respiratory failure due to pulmonary or non-pulmonary diseases. Increases in respiratory effort lead to an increase in oxygen demand further exacerbating hypoxaemia. Animals can quickly become fatigued causing hypoventilation and hypercapnia.
Increased intracranial pressure (ICP). Increases in PaCO2 can trigger cerebral vasodilation resulting in an increased blood flow to the brain, therefore worsening ICP. Such patients may be ventilated in order to maintain a lower PaCO2.
The aims of mechanical ventilation are to increase the excretion of CO2, maximise alveolar oxygenation and reduce the workload of breathing for the patient. The aim should be to normalise cardiovascular parameters and maintain a PaO2 of 80-100 mmHg and a PaCO2 of 35-50 mmHg (Silverstein and Hopper, 2009a), as these are the ranges for patients ventilating normally. The duration of mechanical ventilation will vary depending on the underlying disease process, patient-related factors and case management. Many patients with a disease process that takes time to treat (e.g. tick paralysis) may require ventilation for days to weeks.
It is vital that the veterinary nurse caring for the patient has a clear understanding of the ventilation process, ventilator equipment, individual patient considerations, the underlying disease process, how to troubleshoot problems and the weaning process. Such cases require meticulous clinical records, a dedicated nursing team 24 hours a day and a thorough briefing at shift handovers.
Mechanical ventilators
Ventilators are machines that are programmed to do the work of breathing (either all or some). There are many types of ventilators available for use in clinical settings and it is beyond the scope of this article to give details of them all. They vary considerably in complexity from relatively simple ‘anaesthesia’ ventilators through to modern extremely complex human intensive care unit ventilators (Figures 1, 2 and 3). Depending on ventilator type you will need to select either; a target volume (tidal volume or minute volume) and then check that the generated pressure is not too high, or a target peak inspiratory pressure, and check that an appropriate minute volume is being delivered. The pressure and volume delivered by the ventilator should be checked periodically as changes in the patient's thoracic compliance can lead to alterations in either parameter. If the volume or pressures are too high then there is an increased risk of lung damage (see later) and cardiovascular impairment.
Figure 1. Small animal anaesthesia ventilator.Figure 2. Another type of small animal anaesthesia ventilator.Figure 3. Small intensive care unit ventilator. Courtesy of D Chan, RVC, London.
Getting started
The ventilator should be in a suitable area with oxygen, piped air, anaesthetic machine and adequate gaseous scavenging (if volatile agents are being used). This area should have adjustable lighting, a number of power outlets and be quiet with minimal stimulation. Ideally consumables and laboratory equipment should be near by. A sterile breathing circuit and rebreathing bag should be attached to the outlet flow. The oxygen source should be attached and checked. Alarms and initial settings (Table 1) should be programmed into the machine at this point.
RR
Respiratory rate
8-15 beats per minute. Imitate normal RR
TV
Tidal volume — volume of air in one breath
Patient's bodyweight x volume (8-15 ml)
MV
Minute volume — the volume of air in a minute
TV x RR
PIP
Peak inspiratory pressure — the maximum inspiratory pressure
10-15 cmH20
PEEP
Positive end expiratory pressure — this pressure prevents the alveoli from collapsing therefore reducing the risk of atelectasis (collapsed lung) and improving gaseous exchange
2.5-10 cmH20
I:E ratio
Inspiratory:expiratory ratio
Normally 1:2 to imitate normal breathing
All other consumables including endotracheal (ET)/tracheostomy tube supplies, laryngoscope, plastic tube tie, induction agent/ drug choice and airway suctioning equipment should all be available. The case veterinary surgeon will make a decision on which drugs are to be used to keep the patient sedated/anaesthetised depending on the underlying disease, anticipated length of ventilation, breathing pattern (Table 2) and contraindications.
Mode of ventilation
Description
Controlled ventilation
The patient is reliant on the ventilator delivering every breath. Useful if the patient has paralysis or hyperventilation is required
Intermittent mandatory ventilation (IMV)
A combination of mandatory breaths from the ventilator and spontaneous breaths from the patient. This is often benefcial during the weaning stage
Continuous positive airway pressure (CPAP)
The airway pressure baseline during inspiration and expiration is increased. It is often used during the weaning stage
Low volume ventilation
This method of ventilation is used when there is severe lung disease to minimise additional damage to tissues
Recruitment manoeuvres
These are used to re-expand collapsed alveoli/atelectasis. Positive end expiratory pressure (PEEP) and a high volume of pressure are used for a short period of time to keep the alveoli open
Once the patient is on the ventilator, adjustments to the initial settings will be made based on how the patient is ‘tolerating’ the ventilation and arterial blood gas analysis (PaO2 and PaCO2). Patients should have continuous electrocardiogram, oxygen saturation (SpO2) and end tidal CO2 (etCO2) monitoring which can be achieved using a multi-parameter reader. An arterial catheter should be placed so that invasive blood pressure (IBP) can be measured and multiple drawers for arterial blood gas analysis can be easily collected. Mucous membrane colour, capillary refill time and pulse quality should be checked regularly. Lung auscultation is also important to monitor for problems such as aspiration or pneumothorax. All parameters should be recorded every 15-30 minutes.
Monitoring/troubleshooting
Machines may have integrated alarms that can be programmed depending on the mode of ventilation (Liss, 2012):
Low tidal volume alarms — the breath did not reach the pre-set tidal volume. Common cause is a leak in the system or the endotracheal tube cuff is not inflated fully.
Low pressure alarms — similar to the above. An important factor to consider is pneumothorax as the gas delivered with the breath may be leaking into the pleural space.
High pressure alarms — most likely to occur due to a blockage in the system, also consider the possibility of the patient having developed a tension pneumothorax.
Low SpO2 — move the position of the probe. Consider checking the breathing system for a blockage. Consider increasing the fractional inspired oxygen (FiO2) and checking oxygenation with an arterial blood gas (ABG).
Low or high etCO2 — consider checking the breathing system for a blockage. Assess the respiratory rate and tidal volume and adjust as necessary to maintain a normal CO2.
Low or high blood pressure — check position of equipment (cuff placement if noninvasive blood pressure and transducer position if IBP). Flush arterial line and re-zero transducer. Check other parameters to establish whether there are concurrent changes in heart rate, mucous membranes and capillary refill time.
Nursing considerations
There are a number of nursing considerations for patients on a ventilator:
Eye care — eyes should be fluorescein stained daily to check for the development of corneal ulcers. Ophthalmic lubricant should be applied every 2-4 hours to prevent drying and ulcer formation (Coyer et al. 2007; Silverstein and Hopper, 2009b).
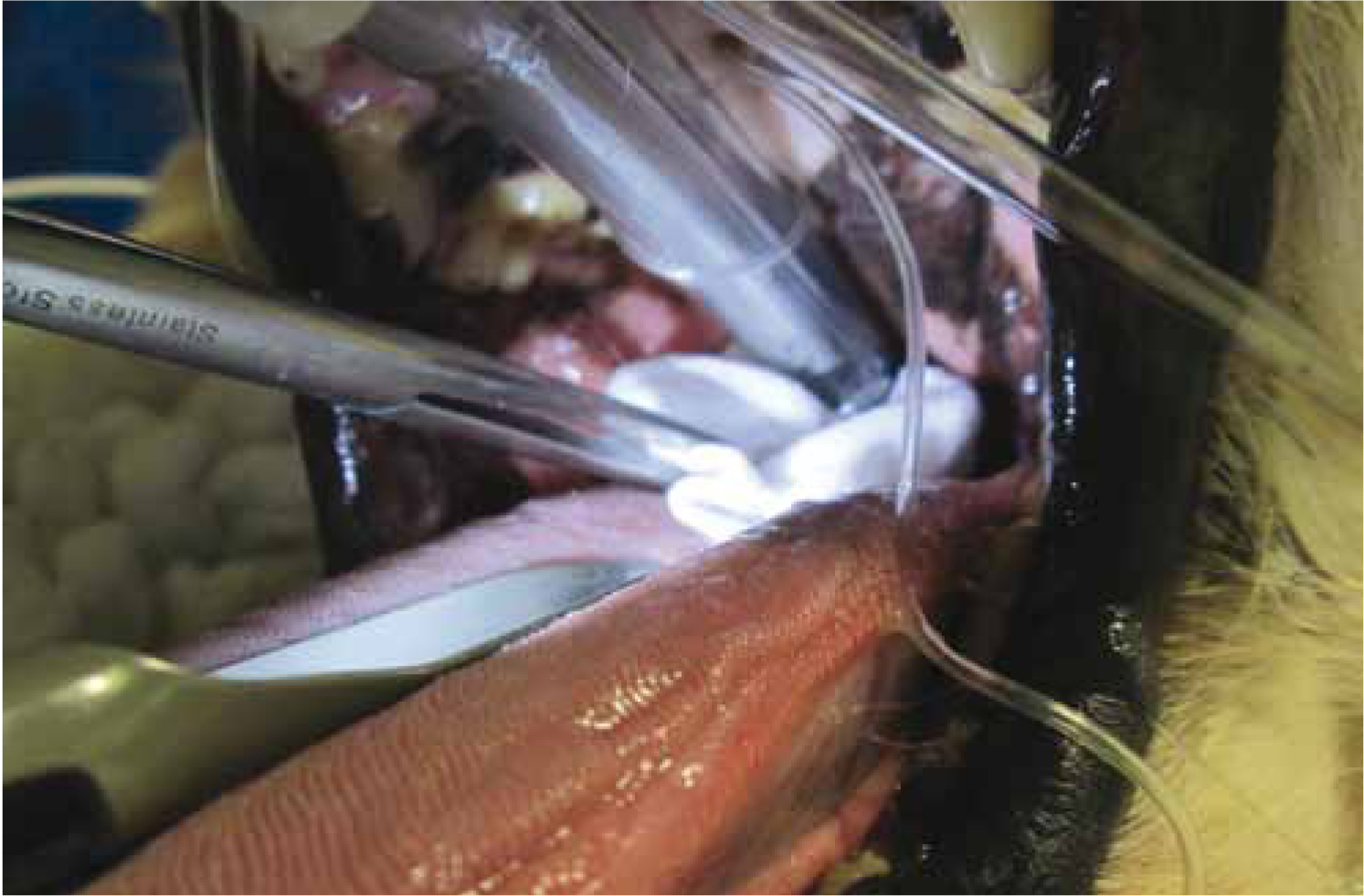
Mouth care — the mouth and oropharynx should be suctioned every 4 hours and a chlorhexidine mouthwash should be wiped around all mouth surfaces to reduce bacterial load (Coyer et al. 2007) (Figure 4). Lingual drying is common and can be counteracted by applying glycerine or covering with a damp swab. SpO2 probes should be repositioned every 2 hours to prevent pressure necrosis. Lingual oedema can develop and so efforts should be made to prevent trauma to the tongue from the teeth and equipment.
Physiotherapy and positioning — recum bent ventilator patients are at risk of pressure sores and muscle atrophy, oedema and nerve damage (Silverstein and Hopper 2009b). Every effort should be made to reduce these developing by turning and micro-repositioning (making small changes to the patient's position) every 2-4 hours. Passive range of movement can be carried out every 6-8 hours to increase lymphatic and fluid movement and to help maintain muscle mass. Positioning can not only help to aid patient comfort but can also help improve oxygenation/ventilation (Coyer et al. 2007). Sternal recumbency is preferred where possible to provide maximal lung compliance. If one lung is affected then the patient can be positioned with the affected lung uppermost to help improve oxygenation (Coyer et al. 2007).
ET tube care/tracheostomy tube care — the ET tube should be suctioned every 4 hours. At this point the cuff should be deflated, the tube untied and repositioned to prevent pressure necrosis (Silverstein and Hopper, 2009b). The ET tube should be changed every 12 hours and tied in place with a plastic tie to prevent bacteria wicking along the tie. Tracheostomy tubes should be managed in the same way as ET tubes. If there is an increased volume of oral secretions the regimen may need to be altered to more frequent suctioning. Care should be taken not to cause hypoxaemia (Couchman et al. 2007).
Humidification — artificial airways lead to reduced filtering and humidification in the upper airway, oxygen is drying and sedation/anaesthesia impairs coughing (Couchman et al. 2007). Heat and moisture exchangers are a suitable solution but must be changed every 24 hours (Silverstein and Hopper, 2009b).
Urination and defaecation — it is vital that ventilator patients are kept clean and dry at all times. Urine output should be 1-2 ml/kg/hour and can easily be monitored with the insertion of a urinary catheter and closed collection system. If a urinary catheter is contraindicated then the bladder should be managed by gentle expression as necessary with the aim of keeping the patient clean and reducing the risk of urine scald. Enemas can be administered as necessary.
Lines, drains and tubes — intravenous catheters, central catheters, arterial catheters, urinary catheters and any other form of tube/drain should be checked at least twice daily for signs of complications. Central lines should be managed aseptically. Feeding tube stomas should be cleaned daily. Urinary catheters should be attached to a closed collection system.
Nutrition — this is always a concern in a ventilated patient. It may be necessary to place a percutaneous endoscopic gastrostomy (PEG) tube, administer partial/total parenteral nutrition (PPN/TPN) or withstand a short period of no nutrition until the animal has been weaned off the ventilator. Lack of nutrition can lead to muscle atrophy and impair ventilator capacity. Overzealous nutritional supplementation with carbohydrates can lead to increased CO2 production (Mellema and Haskins, 2000). Where possible nutrition should be administered to meet at least 50% resting energy requirement. Care must be taken with minimising the risks of aspiration pneumonia (e.g. placing the patient on a slope).
Arterial blood gas analysis — it is important that the veterinary nurse responsible for overseeing the case has a clear understanding of arterial blood gas analysis. Multiple samples will be taken during the initial phases of stabilising the patient on the ventilator and then samples will be repeated at 6-8 hourly intervals (or as necessary) to monitor ventilation.
Treatment of underlying disease — ventilation does not cure the patient, but can allow more time to manage/treat the underlying cause. It is important that treatment is administered as necessary, e.g. medications and monitor electrolytes, packed cell volume and total solids.
Record keeping — all ventilator settings should be recorded at least every hour (Silverstein and Hopper, 2009a). Patient parameters including heart rate, IBP, SpO2 and etCO2 should be recorded every 30 minutes. Temperature should be checked every 4 hours and efforts should be made to prevent hypothermia/hyperthermia. There should be an overlap between staff shift changes so that a full brief can be given to the person taking over the care of the patient (Figure 5). The patient should be given a clinical examination at this time so that they know what parameters are like as they start.
Figure 4. Mouth care — wiping all mucous membranes with a chlorhexidine mouthwash.Figure 5. High dependency set up with two ventilator cases and a dedicated nurse.
Weaning from the ventilator
A decision to try to wean the patient from the ventilator should be made when:
The process requires a reduction in ventilator support until the patient is able to maintain and support their own ventilation. Changes should be made slowly and assessed by monitoring ABGs and patient parameters.
Consideration should be given to the length of time for the patient to ‘wake up’. They may have been mechanically ventilated for some time or been administered drugs such as phenobarbitone that may prolong this time. Patients ventilated for neurological disease may never regain consciousness; those with pulmonary pathology may not recover to the point at which they can be weaned from ventilation.
Complications associated with mechanical ventilation
Ventilator associated pneumonia (VAP) is a common complication (Clare and Hopper, 2005b). These critical patients are often immunosuppressed and at risk of nosocomial infections. Strict oral hygiene and management of the ET/tracheostomy tube are a vital step in reducing the risk of VAP. Elevation of the patient's head and shoulders at 30 degrees may assist in reducing the risk (Coyer et al. 2007).
Ventilator associated lung injury (VALI) is associated with damage to the lung caused by ventilation. Patients with pulmonary disease are at a higher risk of developing VALI. Low volume high frequency ventilation may be selected in high risk patients (Silverstein and Hopper, 2009c).
Conclusion
Ventilator cases should not be embarked on lightly. They require a dedicated nursing team with a good understanding of all aspects of ventilation and individual patient considerations. The long list of patient considerations requires a dynamic approach to ensure that the patient receives the best support available. Ventilator patients can be very rewarding cases when the patient is successfully weaned and their underlying disease process has been treated.
Key Points
There are four main reasons to mechanically ventilate a patient: hypoxaemia, hypercapnia, impending respiratory failure and raised intracranial pressure.
There are a variety of nursing considerations that must be addressed based on the individual.
Ventilation buys a window of time to treat the underlying disease. Not all patients will be successfully weaned from the ventilator.
Common complications associated with mechanical ventilation include ventilator associated pneumonia (VAP) and ventilator associated lung injury (VALI).