Intermittent positive-pressure ventilation (IPPV) is the process of manually or mechanically ventilating a patient that is apnoeic or dyspnoeic. IPPV is a simple and effective method of ventilation, but with complex effects on the body. Nurses should fully understand the method for IPPV and be aware of the implications of poorly performed IPPV.
Intermittent positive-pressure ventilation (IPPV) is the process of manually or mechanically (via a ventilator) ventilating a patient with the use of an endotracheal or tracheostomy tube, and an anaesthetic breathing system. A patient may have difficulty with spontaneous respiration when under anaesthesia due to medication or disease, during thoracotomy or when intra-thoracic pressure is compromised due to a rupture in the thoracic cavity or diaphragm.
Indications of IPPV
Manual IPPV is an inexpensive and effective method of providing regulated ventilation to an anaesthetised patient, both if the patient is unable to spontaneously ventilate, or is having difficulty ventilating sufficiently. Indications for performing IPPV include:
Apnoea (a complete cessation of respiratory effort, potentially due to medication or condition)
To counteract effects of respiratory depression caused by anaesthetic drugs
To provide balanced anaesthesia (the regulation of the ventilation rate and depth of a patient maintains a constant level of inspired anaesthetic gas, and ensures that the anaesthetic plane remains constant)
To reduce respiratory effort in elderly or compromised patients to prevent worsening of their condition
Cardiorespiratory arrest.
Causes of apnoea or hypoventilation include (Hammond, 2007):
Hypothermia
Severe hypoxia
Thoracic surgery or trauma (as breaching of the thoracic cavity will prevent the lungs inflating sufficiently due to an increase in pressure within the pleural cavity)
Anaesthetic agents
Decreased lung, pleural or chest wall compliance
Diseases (e.g. Clostridium tetani)
Central nervous system or spinal cord trauma or disease.
Effects of IPPV on the patient during anaesthesia
Although IPPV appears to be a simple method of ventilation, it has many complex effects on the body. The patient should be closely monitored throughout, particularly with the combined use of capnography and pulse oximetry monitors, to ensure the ventilation provided is appropriate and sufficient.
The effects on the patient and their body system during IPPV include:
Lung ventilation — the extent to which a patient's lung ventilation may be affected depends on the elasticity and resistance of the lungs. Accordingly, anaesthetic gas distribution will vary with the speed at which the lungs are inflated. During respiratory disease where the bronchi are constricted, the resistance of the lungs will be increased (e.g. if the lungs are inflated too rapidly, there will not be enough time for sufficient absorption of oxygen or anaesthetic gases). The inspiratory time should be increased to compensate and allow slow inflation of the lungs. An expiratory pause will be required between each breath to prevent re-breathing and hypercapnia. During disease where the elasticity of the lungs is increased (such as bullous emphysema), care should be taken to prevent rupture of bullae from over-inflation of the lungs (Johnson, 2003).
Cardiovascular function — this is usually depressed during IPPV when compared with spontaneous ventilation. IPPV generally increases intrathoracic pressure (due to an increased inspiratory pressure) which reduces central venous pressure, and venous return to the heart, reducing cardiac output. During hypovolaemia, the venous return is further decreased (Steffey et al, 2015). By decreasing the inspiratory pressure or the time between inhalations, the thoracic pressure will be decreased, which helps to improve cardiac output. Blood pressure should be monitored where possible (Johnson, 2003).
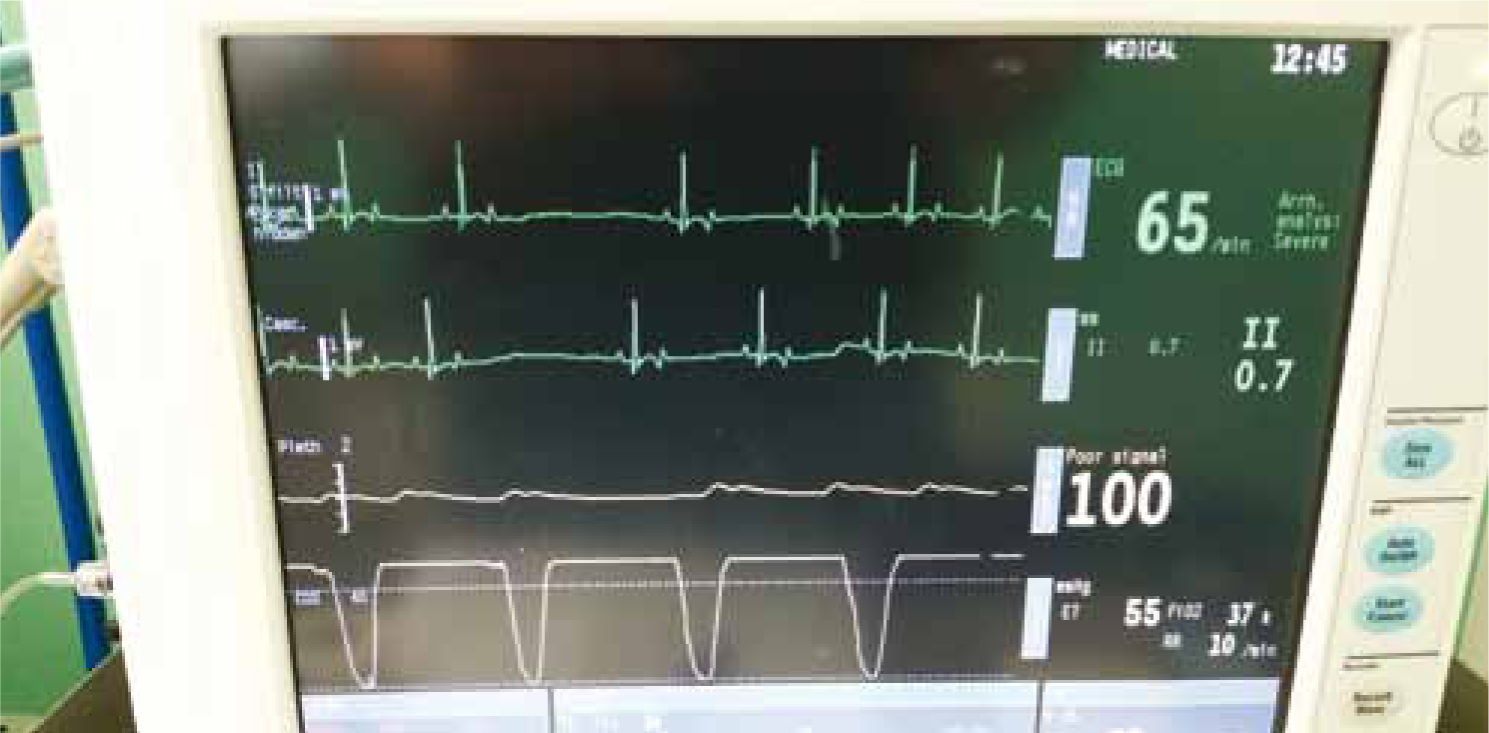
Oxygenation — pulse oximetry (Figure 1) detects the percentage of oxygen saturated in haemoglobin (SPO2) using computer software to measure the absorption of red and infrared light alongside the pulsation of the blood vessel. Assuming that the patient is receiving anaesthetic gas with a sufficient oxygen tension (PaO2), the SPO2 should be 100%. IPPV will mostly improve the SPO2 of a hypoxaemic patient. However, if the cardiovascular system is detrimentally affected by the provision of IPPV, this may cause a reduced tissue perfusion — even if the SPO2 is 100% — meaning that other methods for assessing ventilation should be considered in conjunction with PaO2 and SPO2 (Moens and Coppens, 2007).
Carbon dioxide tension (PaCo2) — in a healthy, non-compromised patient, an increase or decrease in PaCO2 will either spontaneously increase or decrease the patient's respiratory rate and depth to provide normal ventilation. In IPPV, this mechanism is removed, meaning that monitoring the patient throughout is vital. End-tidal carbon dioxide (ETCO2) is measured with the use of a capnograph (Figure 2), which is the most accurate method of ensuring a patient is ventilating sufficiently. Normal ETCO2 is 35–50 mmHg (Hammond, 2007). Hypoventilation and hyperventilation will affect ETCO2 as follows:
Hypoventilation causes an increase in ETCO2, with the patient either re-breathing gas from the anaesthetic breathing system due to a malfunction in equipment or not ventilating enough to remove carbon dioxide. This leads to respiratory acidosis. An increase in arterial blood pressure follows, increasing cardiac workload, and tissue perfusion, leading to increased bleeding at the surgical site.
Hyperventilation causes a decrease in ETCO2, with too much carbon dioxide being removed and respiratory alkalosis occurring, leading to a decrease in arterial blood pressure and tissue perfusion. As oxygen delivery to the tissues is reduced, brain damage can result.
Figure 1. Pulse-oximetry.Figure 2. Normal capnography trace with slightly elevated ETCO2.
It may be difficult to reinstate normal ventilation in a patient following IPPV if a continued hyperventilation (with hypocapnia) has occurred throughout the anaesthesia. This hyperventilation causes a reduced PaCO2, which removes the homeostatic stimulus that assists in normal ventilation (Hammond, 2007).
Anaesthesia — during IPPV, the patient usually requires less anaesthetic agent than when ventilating spontaneously. This is due to the deeper breaths that are usually given to the patient during IPPV than the patient would take if they were breathing on their own. The depth of anaesthesia is often increased more rapidly than during spontaneous ventilation (Dugdale, 2010). Drugs which usually suppress respiration (e.g. some opioids and neuromuscular blocking agents) can be used when IPPV can be performed either manually or automatically. This will reduce the amount of anaesthetic gases required and produce a more balanced anaesthetic (Hammond, 2007).
Complications of IPPV
Complications which may arise when performing IPPV include:
Barotrauma from over-inflation of the lungs
Hypercapnia from inadequate ventilation (leading to respiratory acidosis)
Hypocapnia from excessive ventilation (leading to respiratory alkalosis)
Reduced tissue perfusion from decreased venous return to the heart and decreased cardiac output
Increased intracranial pressure due to increased venous resistance.
Increased personnel and equipment should be used when performing IPPV and monitoring the patient (Clarke et al, 2014).
Which anaesthetic breathing system to use?
When choosing an anaesthetic breathing system, several factors should be considered.
These include:
The size of the patient
The gases being delivered to the patient (noting that care should be taken when using nitrous oxide in a re-breathing system, due to the potential for build-up of nitrogen; oxygen levels should be monitored throughout)
If there is a need to be economical with gas flow
If there is a need to retain heat and moisture
If there will be spontaneous or assisted ventilation (mostly difficult to predict!).
It is ideal to have adjustable pressure limiting (APL) valves (Figure 3) fitted to all anaesthetic breathing systems to prevent excessive pressure within the system and lungs, these should always be kept open during spontaneous respiration (Mosely, 2011).
Figure 3. Adjustable pressure limiting valve on a T-piece circuit.
Manual IPPV method
Prior to anaesthesia, the tidal volume, minute volume and fresh gas flow rate should be determined using the calculation below:
Minute volume (MV) = Bodyweight (kg) x Tidal volume (TV) x Respiratory rate (RR)
A normal tidal volume is usually considered to be 10–15 ml/kg. Multiplying the MV by the anaesthetic circuit factor gives the fresh gas flow (FGF) rate to be used (Table 1).
Circuit
Rebreathing/Non-rebreathing
Fresh Gas Flow for Spontaneous Respiration
Fresh Gas Flow Rate for IPPV
Patient Size
Advantages
Disadvantages
Lack
Non-rebreathing
1 x minute volume (MV)
2 x MV
25 kg+(Mini Lack 2–10 kg)
Cheap and simple to use
Unsuitable for prolonged IPPV
↑FGF (uneconomical)
Long expiratory time needed to prevent rebreathing
Parallel system bulky
Magill
Non-rebreathing
1 x MV
2 x MV
10–80 kg
Cheap and simple to use
Unsuitable for prolonged IPPV
Valve close to patient, access difficulties
Bain
Non-rebreathing
2–4 x MV
1 x MV
10–80 kg
Useful for prolonged IPPV
↓ FGF for IPPV (economical)
Inspiratory gases warmed by expired gases in co-axial tubing
Accidental disconnection of co-axial inner tubing causes re-breathing and increased dead space
T piece (with APL valve)
Non-rebreathing
2.5–3 x MV
2.5-3 x MV
Up to 10 kg
Useful for prolonged IPPV
Ideal for smaller patients
↑FGF rate (uneconomical)
Circle
Rebreathing
100 ml/kg/minute for 10–15 mins then 10 ml/kg/minute
10 ml/kg/minute (alternatively, 0.5–1 l/min for <50kg)
Partially close the APL valve, then squeeze the reservoir bag (ensuring the patient's lungs are not overinflated) and release
Allow a pause for the bag to refill (you may need to increase the flow rate for this) and the patient to fully exhale
Aim for a respiratory rate of 10–12 breaths per minute
When the surgical procedure is complete, reduce anaesthetic gases and decrease the respiratory rate, with spontaneous respiration being stimulated by the increase in carbon dioxide (Prisk, 2014)
Once the anaesthetist is sure the patient is breathing normally, recover as normal, but monitor closely, particularly when the patient is breathing room air to ensure hypoxaemia does not occur (Johnson, 2003).
During cardiopulmonary resuscitation, give the patient two breaths 1 second apart, then give a breath every 3–5 seconds between compressions, using an appropriate anaesthetic breathing system or Ambu-bag. The lungs should be allowed to deflate fully between breaths to promote venous return. 100% oxygen should be used (Beard, 2003).
Mechanical IPPV
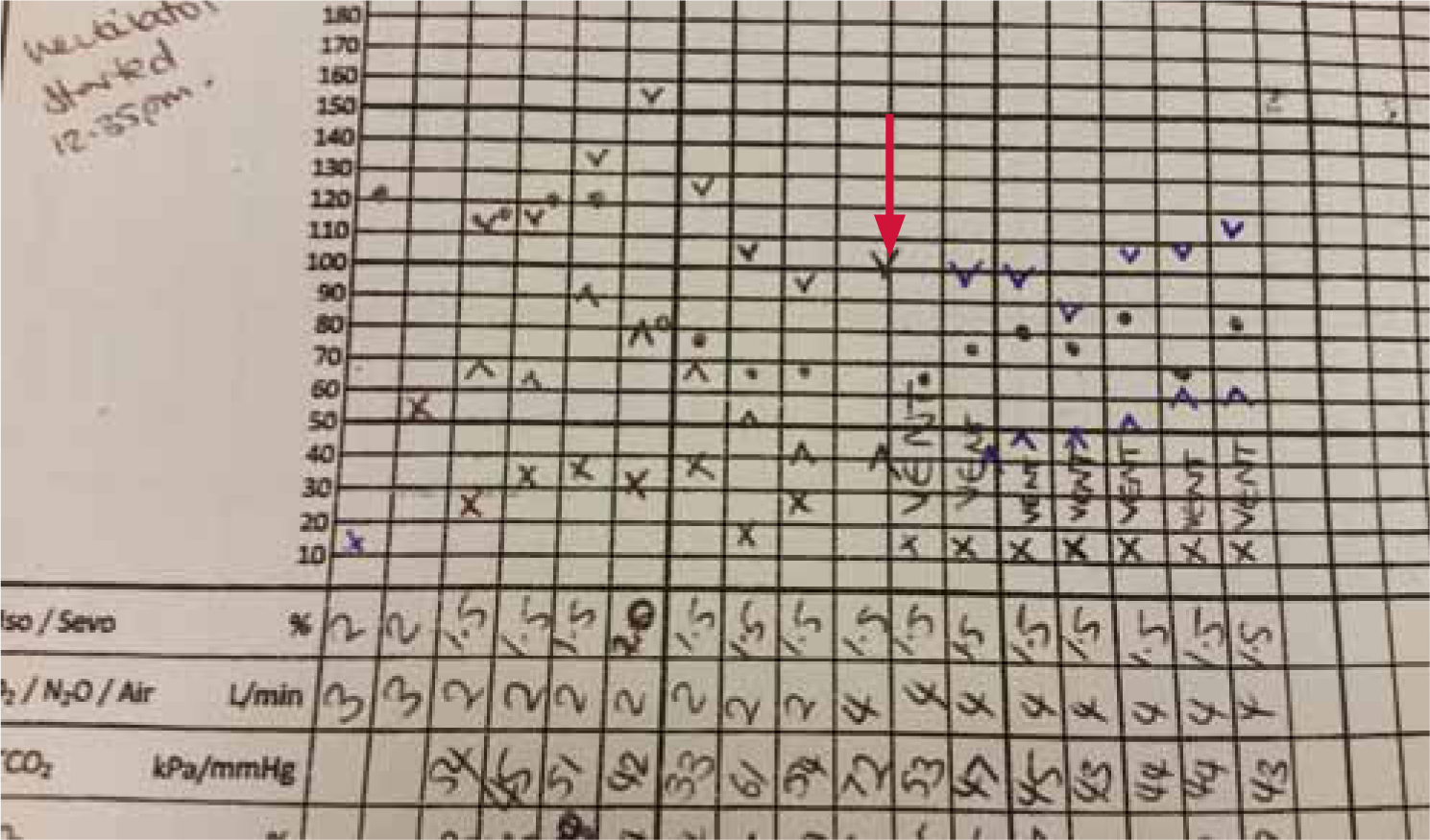
It is possible to provide regulated and accurate IPPV via the use of a mechanical ventilator, though these are very expensive and may be complicated to use. Once the technique is mastered however, there is a great advantage to their use with more regulated IPPV than when IPPV is performed manually. Figure 4 shows the speed with which a patient's heart rate (), respiratory rate (x) and blood pressure (^ and v) become stabilised after an unstable anaesthetic with the use of a mechanical ventilator. Note the decrease in ETCO2 to a normal range once IPPV is initiated.
Figure 4. Rapidly stabilised HR, RR and BP with the use of a ventilator. The red arrow indicates when the ventilator was started. x = respiratory rate, · = heart rate, ^ = blood pressure.
There are differing types of ventilators available, These are as follows:
Volume ventilation — delivers the same tidal volume on each breath and is the most common and simplest to use based on normal respiration. The patient's tidal volume is calculated (using 10–15 ml/kg), and inspiratory and expiratory times are set depending on the respiratory rate required. Some machines will calculate the minute volume from these figures, giving the anaesthetist the fresh gas flow rate. The maximum airway pressure may be adjusted giving the maximum allowed inspiratory pressure, usually 20 cm H20 (Vetronic, 2014).
Pressure ventilation — delivers a set inspiratory pressure of gas. The patient's minute volume is calculated (using bodyweight (kg) x tidal volume x breaths per minute). The inspiratory and expiratory times are set depending on the respiration rate required. The maximum air pressure is adjusted giving the target inspiratory pressure. Pressure ventilation is useful in smaller patients without tight fitting endotracheal (ET) tubes, with leaks compensated for during pressure ventilation, as volume is not the controlling factor.
Timed ventilation — provides inspiration for a set time required to achieve the desired tidal volume. The flow rate is calculated and the inspiratory time is set until the tidal volume is reached. The delivered volume is altered by changing the flow rate. For example, a flow rate of 12 litres/minute with an inspiratory time of 1.0 seconds will give a tidal volume of 200 ml (12000/60 x 1) (Vetronic, 2014).
Modern ventilators combine all three types of ventilation, and any can be used (Figure 5).
Figure 5. Merlin Small Animal Ventilator.
The mechanical and regular cycle of IPPV can in itself inhibit the return to spontaneous respiration. It is possible to wean the patient onto spontaneous respiration with the ‘Assist Mode’ available on some ventilators. However, if this is not available:
Once the need for the patient to remain anaesthetised has passed, switch off the anaesthetic gases and the ventilator, and transfer the patient to a suitable anaesthetic breathing system for manual IPPV
Give the patient 2–3 quick breaths and pause, as the resulting hypercapnia will help stimulate the respiratory centre (the quick breaths will also help break the monotony of the respiration provided by the ventilator)
Continue until spontaneous respiration occurs (Johnson, 2003).
Conclusion
IPPV, whether manual or mechanical, is an efficient method of ventilating patients with apnoea or dyspnoea. Manual IPPV is a useful and cheap method of ventilation. It is difficult to perform correctly and the patient must be monitored appropriately throughout to prevent complications such as hypoxaemia, respiratory acidosis or alkalosis. Mechanical ventilators are efficient and it is much easier to provide the correct values required for the patient. However, they are expensive and may be complicated to use. In each case, the veterinary nurse should be fully educated on the procedures and risks involved before attempting to perform IPPV.