

There are numerous potential side effects to consider when administering anaesthetic inducing drugs. One of the most profound and well-documented side effects is the disruption of the patient's thermoregulatory ability, leading to deviation outside of an acceptable temperature range, resulting in potential derangements in homeostatic processes such as drug metabolism (Clark-Price, 2015). This disruption can result in patient hypo- or hyperthermia. Both have significant negative effects and so it is in the best interests of the veterinary team to minimise and mitigate the occurrence and impact of these conditions. This article will discuss the pathophysiology, effects and methods of prevention and management for hypothermic events in anaesthetised patients. The second part of this series will focus on management and causes of hyperthermia under anaesthesia.
Despite the importance of maintaining normothermia in anaesthetised patients, the definition of ‘normal’ body temperature is poorly defined in veterinary literature, making the goal temperature range ambiguous (Hall, 2021). For the purposes of this article, ‘normal’ temperature ranges are illustrated in Table 1.
Table 1. Normal temperature ranges in small animals (Hall, 2021)
| Species | Temperature Rrange (°C) | Site of temperature measurement |
|---|---|---|
| Dog | 37.2–39.2 | Rectal |
| Cat | 36.7–38.9 | Rectal |
| Rabbit | 37.4–39.6 | Rectal |
Inadvertent perioperative hypothermia
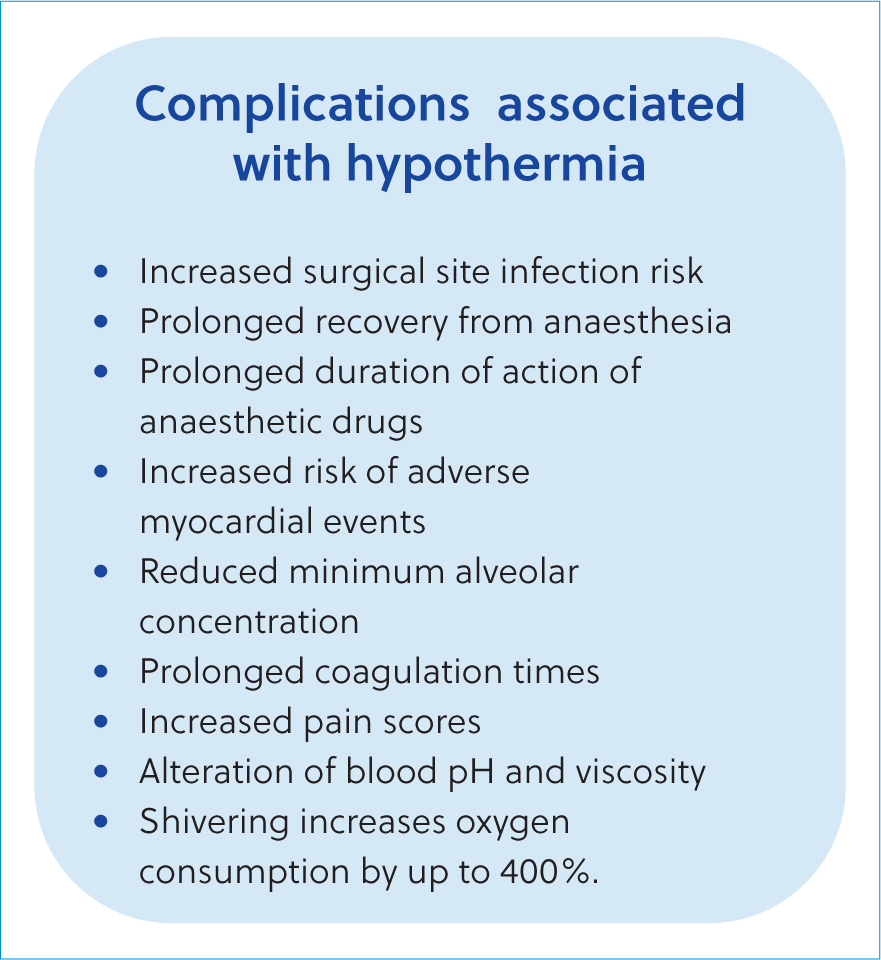
Inadvertent perioperative hypothermia is a common complication of anaesthesia and sedation, although the seriousness of its effects should not be overlooked despite its frequent occurrence (Reynolds et al, 2008). Figure 1 evidences that even minor deviations from normothermia can increase anaesthetic risk and other associated complications (Druce, 2015).
Inadvertent perioperative hypothermia is formally defined as a drop in core body temperature, although the threshold value varies depending on the specific study and species involved (Armstrong et al, 2005; Rose et al, 2016). For the purpose of clarity, this article considers any drop below the patient's ‘normal’ body temperature to be defined as inadvertent perioperative hypothermia, with varying degrees of severity classified in Table 2.
Table 2. Classifications of inadvertent perioperative hypothermia
| Hypothermia severity class | Species | Temperature range °C |
|---|---|---|
| Mild | Dog | 36–37.1 |
| Cat | 36–36.6 | |
| Rabbit | 36.5–37.3 | |
| Moderate | Dog | 35–36 |
| Cat | 35–36 | |
| Rabbit | 35.5–36.5 | |
| Severe | Dog | <35 |
| Cat | <35 | |
| Rabbit | <35.5 |
Measuring patient temperature
When discussing the effects of hypo- and hyperthermia, it is important to specify that these terms relate to deviations in the patient's core body temperature, as peripheral temperature fluctuations are part of the body's normal thermoregulatory process (Davies, 2012). Core temperature can be measured through blood temperature, oesophageal temperature or urinary bladder temperature; each of these methods is invasive and almost certainly require anaesthesia to perform (Hall, 2021). In order to obtain an accurate oesophageal temperature, the probe should be positioned in the distal third of the oesophagus, not the stomach (Rauch et al, 2021). Passing the probe into the stomach may lead to the temperature of the stomach acid being mistaken for core temperature (often lower than core temperature) or can facilitate leakage of gastric contents into the distal oesophagus as the probe will prevent the cardiac sphincter from closing fully (Rauch et al, 2021).
In conscious patients, rectal thermometry can provide relatively accurate results, although care should be taken to consider the influence of faecal matter, gas and probe positioning, as intestinal temperature tends to read higher than rectal temperature, meaning that depth of probe placement will impact the result (Hall, 2021). Aural temperatures can be a reliable alternative to rectal temperature in dogs if used properly, although it should be noted that readings must be interpreted using the ear specific reference range (36.6–38.8°C) and cannot be used interchangeably with rectal temperatures (Hall, 2021).
Methods of heat loss and patient impact
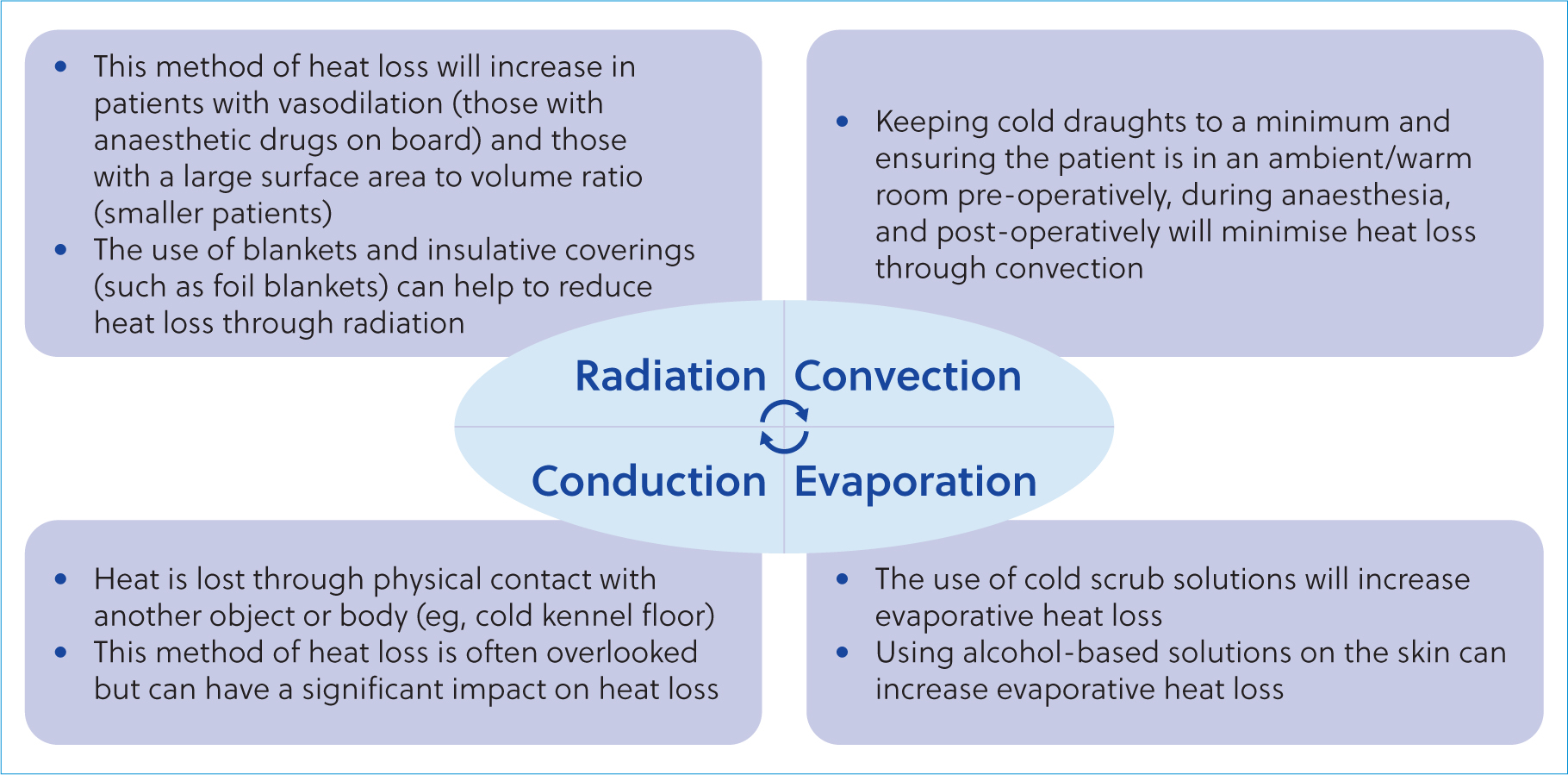
Whilst hypothermia is a side effect commonly understood to be related to anaesthetic events, the consequences of such are often overlooked, underestimated or misinterpreted as ‘normal’ post anaesthetic responses (Bowers, 2012). Heat can be lost through several different mechanisms (Figure 2). It is vital for the veterinary team to be aware of these various methods, as mitigation and prevention covering all methods is the only effective way to combat inadvertent perioperative hypothermia.
Heat loss occurs in three distinct phases: redistribution (phase I), linear phase (phase II), and plateau phase (phase III). These phases are illustrated in Figure 3.
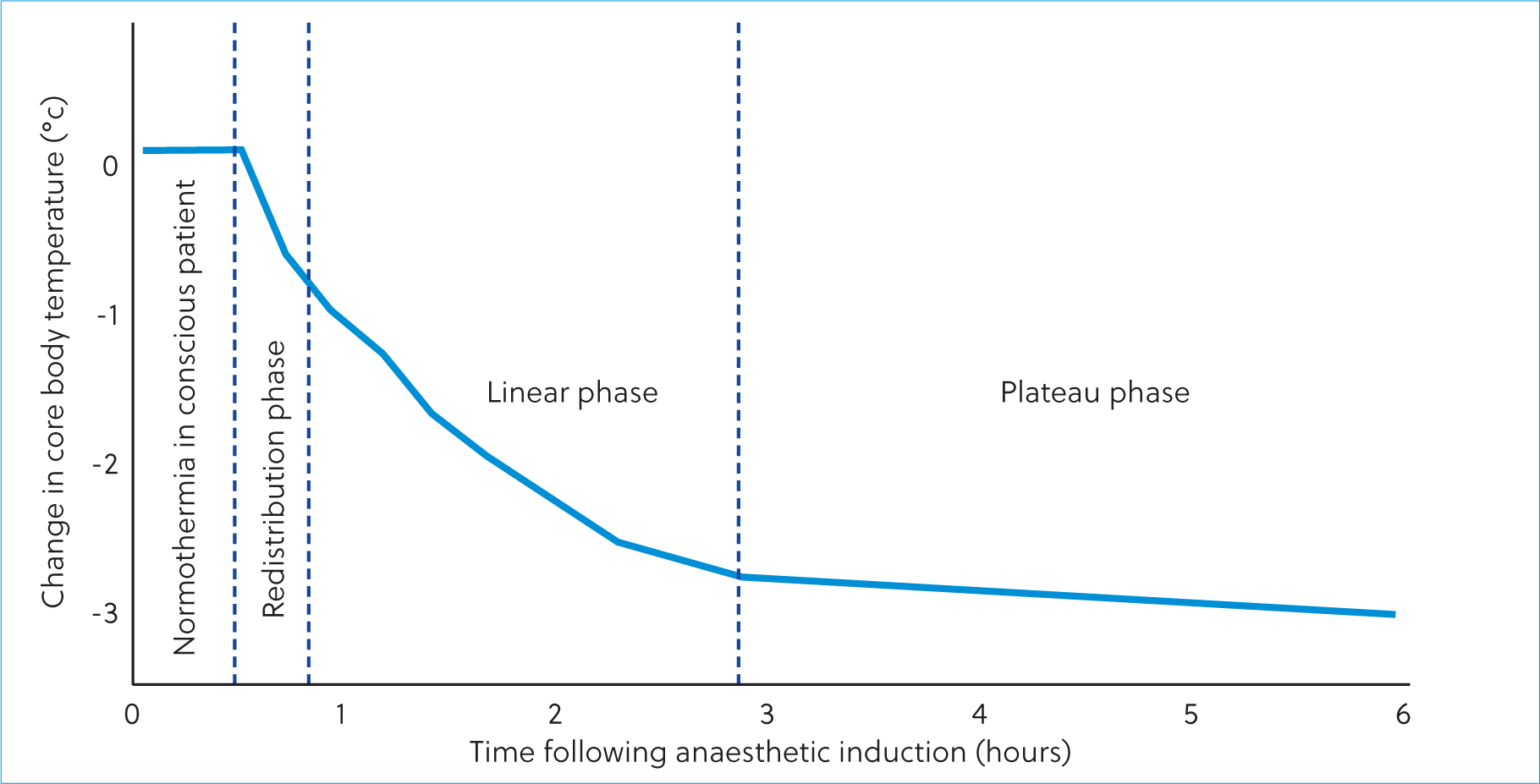
Anaesthetic drugs impair the body's ability to thermoregulate; therefore, vasodilation induced by the administration of these drugs encourages redistribution of heat from the core to the periphery, thereby initiating the redistribution phase (Rauch et al, 2021). Similarly, whilst Figure 3 indicates that low core body temperatures are not reached until the anaesthetic period is prolonged, the use of cold surgical scrub, the absence of warming aids, extensive clipping and anaesthetic drug dose and choice can all increase the speed at which the patient loses heat. Patient size, haemodynamic status and body condition score can all impact the speed of heat loss during the linear phase; therefore, patients undergoing short anaesthetics are just as vulnerable to inadvertent perioperative hypothermia as those undergoing longer procedures (Rauch et al, 2021). Most notably, the lower the gradient between the core and periphery temperature, the lower the redistribution rate and the lower the drop in core temperature (Rauch et al, 2021). In short, patient's experiencing pyrexia will lose heat rapidly when anaesthetised and so their risk of inadvertent perioperative hypothermia should not be overlooked.
Anaesthetic overdose
Some anaesthetic drugs, such as isoflurane, will cause a dosedependent vasodilation, meaning that higher doses of the drug are more likely to exacerbate hypothermia. Similarly, patients that are hypothermic have a reduced minimum alveolar concentration, which initiates a self-perpetuating cycle of relative anaesthetic overdose leading to hypothermia, furthering the relative anaesthetic overdose (Liu et al, 2001; Ruetzler and Kurz, 2018; Thompson and Murrell, 2018). If left uninterrupted, this self-perpetuating cycle can lead to cardiorespiratory arrest (Reynolds et al, 2008).
Altered pharmacodynamics
In cases of moderate to severe hypothermia, drug metabolism may be altered due to changes in blood pressure, reduced tissue perfusion, altered protein metabolism, altered enzyme efficacy or bradycardia (Giuliano and Hendricks, 2017; Thompson and Murrell, 2018). This can lead to patients being unable to efficiently metabolise drugs that are vital to their recovery (such as analgesia) and prolong post-operative hospital stays, increasing practice labour and patient care costs (Giuliano and Hendricks, 2017). In a case outlined by Thompson and Murrell (2018), a patient undergoing surgery experienced a bradycardic event during anaesthesia that was unresponsive to two doses of glycopyrrolate. The authors of this case postulate that the patient's severe hypothermia may have impacted the drug's efficacy. Studies in human anaesthesia support this theory, as enzyme activity is highly temperature sensitive, meaning that significant changes to the body's core temperature will impact the metabolism of drugs (Reynolds et al, 2008). Similarly, reduced blood flow to organs such as the liver and kidneys will prolong drug metabolism leading to slower onset of action, and potentially prolong recovery from anaesthesia (Bowers, 2012).
Coagulation derangements
Factors such as platelet function, clotting factor enzyme function and fibrinolytic activity are all impacted during inadvertent perioperative hypothermia events potentially leading to increased intraoperative blood loss (Reynolds et al, 2008). These disturbances in the clotting cascade are unable to be predicted through pre-anaesthesia clotting profiles as the tests are performed using blood taken from normothermic patients (Hart et al, 2011). Patients experiencing inadvertent perioperative hypothermia may also become hypercoagulable as a result of the perturbations to the clotting cascade (Rauch et al, 2021).
Adverse myocardial events
Due to a combination of peripheral vasoconstriction, altered tissue perfusion, inhibition of normal enzyme activity and coagulopathies, hypothermia can lead to cardiac arrhythmias, myocardial ischaemia, and even cardiorespiratory arrest (Giuliano and Hendricks, 2017). Brodbelt et al (2008) outlined a link between inadvertent perioperative hypothermia and an increase in morbidity, particularly in smaller patients where heat loss is exacerbated by their large surface area to volume ratio. One potential reason for this, is that inadvertent perioperative hypothermia induces heat conserving responses from the body, such as shivering. Shivering increases the patient's oxygen demand by 50–400% and it is entirely possible that patients with cardiopulmonary disease (or compromise caused by anaesthetic drugs) cannot fulfil these increased metabolic demands (Reynolds et al, 2008; Hart et al, 2011; Bowers, 2012). In human medicine, a drop in temperature just 1°C below normothermia can activate release of ‘stress hormones’ such as adrenaline and noradrenaline, leading to increased cardiac workload and can increase the incidence of adverse myocardial events (such as arrest) in patients with concurrent cardiovascular disease (Hart et al, 2011). Once myocardial requirements surpass the body's ability to fulfil this demand, tissue perfusion is compromised, leading to reductions in cerebral blood flow (Davies, 2012).
Post-operative infection rates
Several studies demonstrate the role of hypothermia on surgical site infection (SSI) rates in human medicine (Kurz et al, 1996; Seamon et al, 2012; Mann, 2015; Rauch et al, 2021). A study by Beal et al (2000) found no significant link between hypothermia and SSI incidence; however, the threshold temperature used to define hypothermia was 37.8°C, significantly higher than some of the low end ‘normal’ temperature ranges that Hall (2021) discusses, which will have likely impacted the results.
In humans, SSI incidence may be increased in hypothermic patients due to peripheral vasoconstriction leading to decreased subcutaneous oxygen tension; the incidence of SSIs is correlated with subcutaneous oxygen tension (Reynolds et al, 2008; Rauch et al, 2021). It is also hypothesised that hypothermia may impair neutrophil function through direct and indirect means, reducing the body's ability to mount an immune response against pathogens (Reynolds et al, 2008; Rauch et al, 2021). Some studies suggest inadvertent perioperative hypothermia can increase SSI risk by more than six times (Rauch et al, 2021). In an age where antimicrobial resistance is one of the biggest threats to the One Health directive, prevention of SSIs is a relevant and necessary contribution from the veterinary profession (Hernando-Amado et al, 2019).
Prevention and mitigation techniques
Having discussed the importance and mechanisms behind inadvertent perioperative hypothermia, methods of mitigation and prevention are explored here. It should be remembered that the prevention of hypothermia is of greater patient benefit than allowing inadvertent perioperative hypothermia to set in and correcting it at a later time. Establishing the patient's pre-anaesthesia temperature is a key part of reducing inadvertent perioperative hypothermia, although this may not be possible for all patients due to fear, stress or other influencing factors (Grubb et al, 2020; Hall, 2021). If the patient is not normothermic prior to anaesthesia, this should be discussed within the veterinary team and the urgency of anaesthesia considered prior to temperature stabilisation (Grubb et al, 2020).
Passive strategies and aids
Passive heating aids help to prevent temperature loss but do not add heat to the patient. Use of blankets, bubble wrap, foil blankets, socks, and Medical Pet Shirts can all help to reduce heat loss during the redistribution phase by decreasing convection losses (see Figure 4). These devices can be used throughout the anaesthetic period, but they will not warm patients that are already cold (Bowers, 2012). The use of foil blankets in the recovery phase should be carefully considered. Due to their loud noise, this may exacerbate emergence delirium (author's experience). Unless the anaesthetic period is to be exceptionally brief, the use of passive heating aids alone is rarely sufficient to maintain normothermia under anaesthesia, particularly in surgical cases (Bowers, 2012). Passive heating aids and strategies are easily implemented in veterinary practice due to the low financial cost, versatile application, and convenience.

Active heating aids
Active heating aids help to reduce temperature loss through warming the air around the patient, thereby reducing the temperature gradient between the body's surface and the environmental temperature (Bowers, 2012; Redondo et al, 2012). Forced air warming (FAW) devices such as the BairHugger™ present an initial cost to the veterinary practice but are consistently successful at maintaining normothermia and preventing hypothermia in a plethora of clinical studies (Machon et al, 1999; Hart et al, 2011; Bowers, 2012; Davies, 2012; Redondo et al, 2012; Epstein et al, 2013; Giuliano and Hendricks, 2017; Rauch et al, 2021). The risk of thermal injury when using FAW devices correctly is minimal, and reusable blankets are available, making them a more environmentally sustainable option when compared to units using disposable blankets (Bowers, 2012). The use of FAW devices during surgical procedures has previously been linked to an increase in SSIs; however, research has disproven this theory (Huang et al, 2003; Bräuer and Scheithauer, 2016). FAW devices can be utilised intraoperatively with minimal inconvenience to the surgeon if switched off until the surgical field has been draped (Davies, 2012).
Electric heat mats are also available for supplementary active heating. Some mats are pressure sensitive and so require the patient's weight on them before they generate heat, whilst other mats can be used both above and beneath the patient during the anaesthetic period (Kibanda and Gurney, 2012; Potter et al, 2015). Direct contact between the mat and the patient should be avoided to reduce the risk of thermal injury and their use in conscious patients should be carefully considered due to the risk of the patient chewing through the wires (Hart et al, 2011; Bowers, 2012; Mann, 2015). Similarly, their use in anaesthetised patients should be carefully monitored as the patient has no ability to remove themselves from the heat source (Bowers, 2012). Heat mats may be of limited usage below particularly heavy patients, as recumbency can compress peripheral vessels that would otherwise distribute heat through the body (Mosing, 2016). Despite these multiple considerations, electric heat mats are an effective adjunct to the veterinary nurse's arsenal against hypothermia.
The use of intravenous fluid warmers is hotly debated in some older literature; however, when used correctly, fluid warming has shown to be efficacious in preventing hypothermia (Leben and Tryba, 1997; Hart et al, 2011; Davies, 2012; Dendis and Hooven, 2020). The use of fluid warmers as a sole warming agent is not recommended as the temperatures required of the machine would cause cell lysis (Hart et al, 2011). Their role in inadvertent perioperative hypothermia management is to prevent further temperature decrease, not to warm the patient (Mann, 2015).
‘Hot hands’, hot water bottles and microwavable heat discs are a low budget option for patient warming although each comes with its own associated risks. ‘Hot hands’ is a colloquial term referring to latex gloves filled with warm water. In some instances, the patient may accidentally burst the ‘hot hand’, risking patient burns, or at least wetting the patient, and causing further heat loss. In the absence of a fluid warming device, wrapping the fluid giving set around a ‘hot hand’ will provide some additional warmth to the fluid being administered (Bowers, 2012). Hot water bottles lose heat at around 5°C per hour and can act as a heat sink once they reach the patient's body temperature (or below), as well as posing a risk of thermal injury (Tan et al, 2004; Druce, 2015). Microwavable heat discs are commercially available for the purpose of patient warming. These discs are extremely useful when needing to provide ‘in kennel’ warming aids as they are robust, soli, and durable. However, used without coverings, thermal injury can occur and due to the nature of microwaves, can develop an uneven heat distribution (Druce, 2015). Whilst these devices are favourable due to their ease of use and low cost, the inability to regulate or accurately measure their temperature alongside the potential for thermal injury means that their usage is only truly indicated in the absence of FAW devices.
The impact of medical gases (such as oxygen and medical air) on patient core temperatures varies depending on the patient's fresh gas flow rate, and the type of anaesthetic circuit used (rebreathing or non-rebreathing) (Hart et al, 2011). The impact of heat and moisture exchangers in combatting hypothermia is minimal, particularly as a lone intervention (Hart et al, 2011).
Conclusions
Inadvertent perioperative hypothermia is a common complication of anaesthesia that brings with it a host of detrimental patient effects. However, the veterinary team have tools at their disposal in order to combat and prevent its insidious onset. Preventing a patient from becoming hypothermic is much more cost effective, less time consuming, and more beneficial to the patient, than correcting an already established hypothermia. The role of the veterinary nurse is often synonymous with that of a patient advocate, therefore the role of the veterinary nurse in the management and prevention of hypothermia is integral.
KEY POINTS
- Inadvertent perioperative hypothermia is a commonly overlooked complication of anaesthesia in companion animals.
- Hypothermia can disrupt normal homeostatic processes leading to coagulopathies, cardiac ischaemia, increased surgical site infection risk and cardiorespiratory arrest.
- Most heat loss occurs within the first hour of anaesthesia.
- Using a combination of active and passive heating aids, hypothermia can be prevented and its effects minimised.
- Prevention of hypothermia is of greater benefit to the patient than correcting an already established hypothermia.