

The canine elbow is a complex joint composed of the humerus, ulna and radius. The articulating regions of these bones are the radial head, ulna trochlear notch, anconeal process, medial and lateral coronoid processes of the ulna and the trochlea, capitulum and supratrochlear foramen of the humerus. Together these bones form a hinge made up of three smaller synovial joints. All three of these joints serve different purposes. The humeroradial joint transmits most of the weight bearing, the humeroulnar restricts the movement of the joint to flexion and extension and the radioulnar joint allows rotational movement.
Elbow joint disease is a relatively common diagnosis in dogs and has a high welfare impact as evidenced by the high proportion of cases recorded with pain, lameness and analgesic therapy (O'Neil, 2020). Canine elbow dysplasia is a term encompassing multiple developmental anomalies of the cubital joint, including elbow incongruity, a fragmented medial coronoid process, an ununited anconeal process, osteochondritis of the humeral condyle and ununited medial epicondyle (Burton and Owen, 2008).
However, because of the wide variety of pathologies commonly encountered in dysplastic elbow joints and the ongoing debates over their aetiology, the term elbow dysplasia may not be ideal and the term ‘developmental elbow disease’ has been proposed as a more appropriate umbrella term for these different but interrelated conditions.
‘Incongruity ‘is a term describing anatomical malalignment of the surfaces of a joint. Developmental incongruity of the elbow has been suggested as a mechanism that may lead to elbow dysplasia (Burton and Owen, 2008). Three types of joint incongruity have been demonstrated: radioulnar length mismatch; humeroulnar incongruity; and radioulnar incisure incongruity (Burton and Owen, 2008). The abnormal conformation of the elbow joint, or incongruity, results in the humerus, radius and ulna fitting together in a way that leads to areas of abnormally high contact pressure. This abnormal pressure can lead to the following different problems which may or may not occur in the joint at the same time:
- Fragmented medial coronoid process (FCP) (also known as medial coronoid process disease MCPD) — FCP and joint incongruence are the most commonly documented pathologies within the medial elbow joint compartment (Krotscheck and Bottcher, 2018). In this condition the medial coronoid process of the ulna develops a fissure and separates from the rest of the ulna (Figure 1), resulting in pain and instability. It is the most common dysplastic lesion of the elbow shown to be the main cause of lameness in the majority of studies (Burton and Owen, 2008).
- Osteochondritis dissecans (OCD) — osteochondrosis is a pathological condition in which normal endochondral ossification is disturbed. The result is abnormally thick regions of cartilage that are less resistant to mechanical stress, when compared with the stronger and denser bone. The abnormal development of the articular cartilage covering the humeral trochlea and its failure to turn to subchondral bone causes it to crack, fissure and form a flap or osteochondritis dissecans lesion. These lesions are most commonly found in male Labrador retrievers (Burton and Owen, 2008). Predisposing factors are thought to include diets rich in energy, calcium and phosphorous, accelerated growth, intense exercise, and increased birth weight (Burton and Owen, 2008).
- Ununited anconeal process (UAP) — in some breeds, the anconeal process develops from a separate centre of growth to the rest of the ulna (Figure 2), but the two parts fuse together at around 4 months of age. Ununited anconeal process is a disease characterised by failure of the anconeal process to fuse with the diaphysis of the ulna in young growing dogs (Shales, 2006). Predisposition to this condition is seen primarily in fast growing large breed dogs, with German Shepherd dogs having the highest reported incidence (Shales 2006). There are many theories for the aetiology of UAP, including trauma, genetics, growth plate trauma associated with growth retardation and asynchronous growth between the radius and ulna.
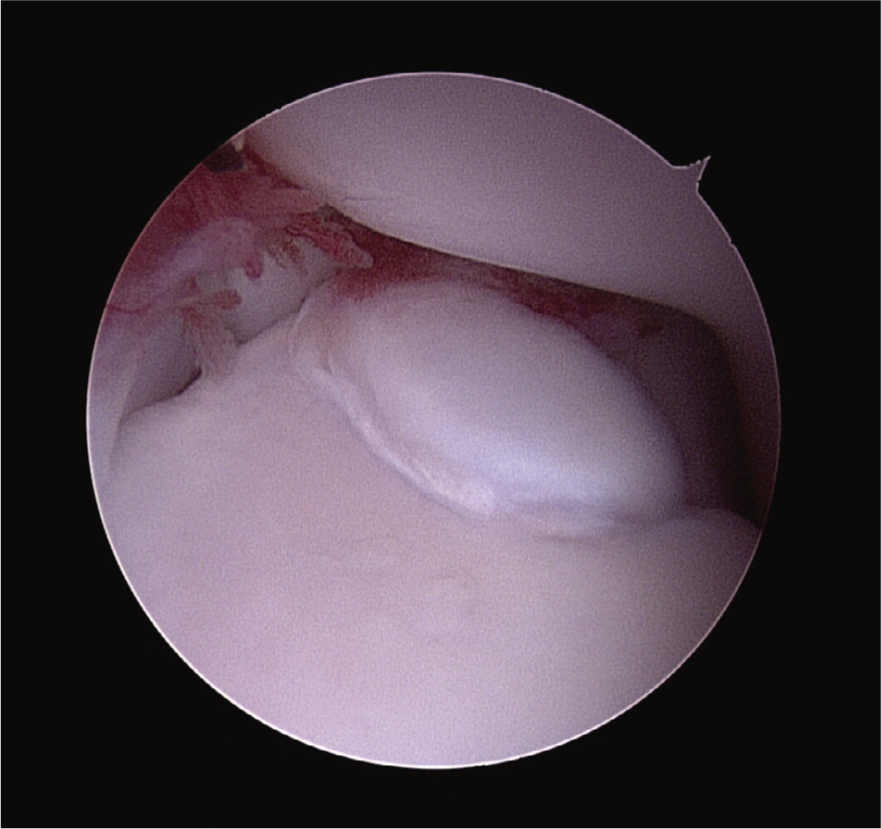
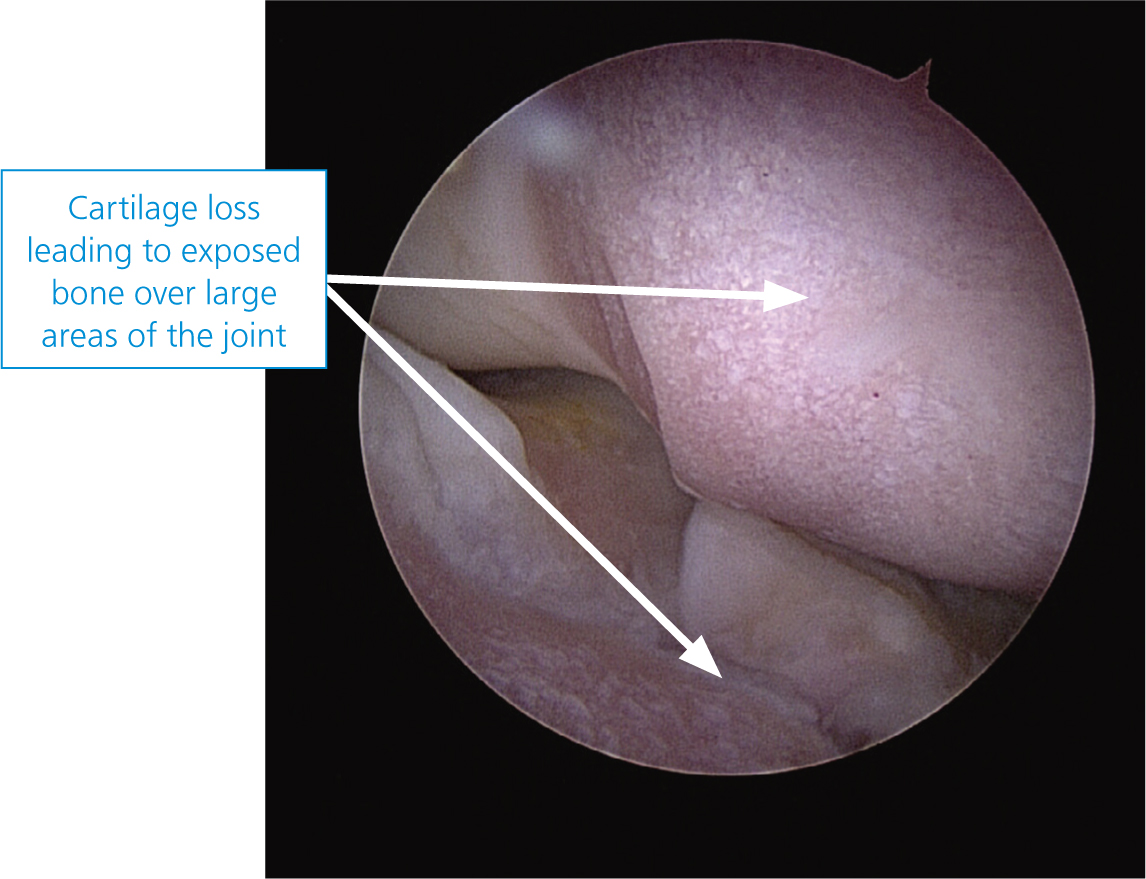
- Medial compartment disease (MCD) — occurs as a result of developmental elbow disease. Extensive cartilage loss in the medial compartment (Figure 3) occurs most frequently in adult and old dogs (Coppieters, 2015). A percentage of dogs develop more extensive overloading of the medial joint compartment, leading to a diffuse loss of cartilage of the entire coronoid process and the opposing humeral trochlea. As a result, the inside part of the joint collapses with eventual grinding of bone on bone. However, the lateral part of the elbow joint appears normal in the vast majority of patients.
- Ununited medial epicondyle — now known as flexor enthesopathy. Although it can affect patients with preexisting elbow disease or occur as a primary disease, it is typically not currently recognised in the developmental elbow disease complex, so will not be covered in this article.

Diagnosis
The most common age for onset of clinical signs of developmental elbow disease is between 6 to 10 months of age, however some dogs only present as middle aged or older adults when they have advanced osteoarthritis.
Signs of developmental elbow disease
There are a number of signs of developmental elbow disease, and regardless of the exact cause the clinical signs are the same.
- Lameness in one or both forelimbs
- Stiffness, especially after lying down
- Reluctance to exercise
- Often the forelimbs appear turned out
- Difficulty coming down stairs
- Joint swelling and pain on clinical examination
- Restricted range of movement as the joint becomes thickened
- Sometimes there are, however, no findings on palpation/manipulation
- All conditions associated with medial compartment disease result in lameness of varying degrees and pain with manipulation of the elbow joint. The lameness, however, can be difficult to notice because often it is bilateral and young dogs may remain active despite their joint pathology.
Intra-articular local anaesthesia can also be used to identify a painful joint. The patient is sedated, synovial fluid is removed, and then local anaesthetic is inserted. The dog is then observed to evaluate the effects on lameness. The block may temporarily resolve signs of lameness caused by synovitis, osteochondral lesions, and cartilage erosions. A study by Van Vynckt et al in 2012 on lame dogs showed a positive effect in 87% of the dogs injected, a false negative in 10%, and a true negative in 3% of dogs which indicated the technique was reliable in 90% of the cases (Van Vynckt et al, 2012).
Imaging
Imaging is important in cases of canine elbow disease in order to provide diagnosis and determine treatment options as well as to provide prognostic information to the client. The imaging options available are radiography, ultrasonography, computed tomography (CT) and magnetic resonance imaging (MRI). Nuclear scintigraphy is also an option, although this is not widely available in small animal practices. MRI is regularly used in human medicine to detect osteoarthritic changes. In contrast to human joints, MRI of canine joints is not routinely used to visualise cartilage. Due to the low resolution of most currently available MRI devices in veterinary medicine, the opposing thin cartilage layers of the canine elbow cannot be clearly differentiated.
Widely available, efficient, and cost effective, radiographic assessment is a valuable component of the diagnosis of elbow disease However, studies have shown a lack of sensitivity for standard radiographic techniques compared with CT. A study by Punke et al (2009) concluded that forelimb lameness can be caused by elbow pathology that is not detectable by conventional radiographic projections and that scintigraphy and CT are more sensitive than standard 3 radiographic projection examinations for detection of elbow pathology. This is because of the two-dimensional nature of radiographic projections and the complex three-dimensional anatomy of the elbow joint and the wide spectrum of pathology involving the cartilage and/or bone (Cook and Cook, 2009). This anatomy leads to the superimposition of structures. For example, in the case of osteochondral fragments, although oblique projections of the canine elbow have been suggested to increase the sensitivity for identifying fragmentation of the medial coronoid process no radiographic projection is able to demonstrate the axial border of the medial coronoid process without superimposition of other bony structures (Moores et al, 2008). Therefore, medial coronoid disease is often diagnosed radiographically from the presence of secondary joint changes. The diagnosis of incongruity by conventional radiography is also insensitive (Michelsen, 2012).
CT is seen as superior to radiography in diagnosing elbow disease (Lau et al, 2015) and can be performed rapidly under sedation rather than general anaesthesia. It can provide detailed cross-sectional images of the bony structures of the elbow without superimposition, meaning that FCP and OCD lesions can be identified. Assessment of elbow incongruity has benefited from advanced imaging techniques such as CT as the multiplanar reconstruction of images means the relationships between the radial and articular surfaces can be assessed. However, CT images have good bone detail but cannot be used directly to differentiate cartilage from other soft tissue structures. Therefore, neither radiography nor CT alone can directly identify cartilage erosion (Moores et al, 2008).
Arthroscopy requires general anaesthesia but allows visualisation of joint surfaces and therapeutic interventions at the same time. Arthroscopy is also important for the assessment of the severity and extent of cartilage pathology, as this cannot be appreciated using CT alone. However, arthroscopy alone cannot identify all lesions present. In a study by Moores et al (2008), CT identified incomplete fissure fractures, which prompted burring of the medial coronoid process to reveal fragmentation hidden under grossly normal articular cartilage. Their study identified lesions in eight elbows that would have been missed by arthroscopy alone.
Therefore, arthroscopy complements CT findings, facilitating the treatment decision process. CT displays bone but not cartilage and arthroscopy enables observation of the articular cartilage but not the subchondral bone (Moores et al 2008).
A variety of protocols are suggested for the radiographic assessment of the canine elbow joint. As a minimum a craniocaudal and a flexed mediolateral view are recommended. For a complete radiographic assessment of the elbow joint, four radiographic projections are required (Cook and Cook, 2009) (Table 1).
Table 1. Radiographic views of the elbow joint
| Radiographic view | Technique | Important areas to assess and potential pathology |
|---|---|---|
| The dog is positioned in sternal recumbency with the affected limb pulled cranially. The dog's head is turned away from the side of interest and supported on a foam block. Rotating the trunk towards the side of interest may help to keep the extended limb straight. The limb should be placed directly on the x-ray cassette. To centre palpate the humeral epicondyles. Collimate to include the skin margins and one third of the humerus and antebrachium |
|
|
| The dog is positioned in lateral recumbency with the affected limb directly on the x-ray cassette. A foam wedge is placed under the scapula to help lift the thoracic spine and position the elbow laterally. The affected limb is pulled cranially with the use of ties and sandbags and the elbow flexed to approximately 45°. The unaffected limb is tied and pulled caudally so that it lies along the thorax. To ensure there is no rotation palpate to ensure the humeral epicondyles are aligned vertically. A small foam pad can be used to support the carpus if needed. Centre at the level of the humeral condyle and collimate to include the adjacent third of the humerus and antebrachium |
|
|
| Extended mediolateral view | Position as for the flexed view but secure the elbow in extensions (approximately 120° to 150°). Centre and collimate as for the flexed lateral view | In addition to the areas described for the flexed view:
|
| The dog is positioned as in a craniocaudal view. Rotate the limb medially by 15° and secure with sandbags. Centre at the level of the humeral condyle and collimate to include one third of the adjacent humerus and antebrachium | Medial coronoid process of the ulna for identification of coronoid fragments |
Diagnosing osteochondrosis
OCD lesions can be identified on lateral and craniocaudal radiographs but are generally best identified on craniocaudal or cranial 15° lateral–caudomedial oblique projections (Cook and Cook, 2009). The lesions occur almost exclusively on the weight bearing surface of the distal medial condyle. OCD can be observed as radiolucency, flattening, irregularity or defect in the subchondral bone. Some cases may have concurrent OCD and FCP, so diagnostic arthroscopy is useful.
Diagnosing FCP
Diagnosis of an FCP can be challenging as the coronoid process is difficult to image radiographically and a discrete fragment is rarely visible (Burton and Owen, 2008). This is because the fragments tend to displace laterally where they are obscured by the radial head (Barrett, 2008). Looking for other changes that may have occurred as a consequence of the FCP lesion may be more useful. These include osteophytosis (the formation of osteophytic growths or bone spurs) of the radial head, anconeal process and medial aspect of the trochlear notch, sclerosis of the ulnar trochlear notch and sometimes joint effusion. The use of a 15° craniolateral-caudomedial view may sometimes be useful in identifying the fragment but in many cases, diagnosis will require arthroscopic or CT examination of the joint.
Diagnosing UAP
Dogs with UAP generally present with chronic lameness which is worse post exercise. Joint effusion can be detected with palpation and a pain response elicited during palpation of the region and extension of the joint. UAP can usually be confirmed by radiography with a flexed mediolateral view proving the best visualisation of the anconeus.
Conclusion
Imaging is important in dogs showing signs of elbow disease in order to identify the disease processes present and to implement an appropriate treatment plan. However, no single non-invasive diagnostic procedure can identify all the pathological changes present with complete reliability. Therefore, a combination of CT and arthroscopy is recommended to visualise the surface of the joint and identify the presence of fissures, chondromalacia and fragmentation as well as the presence of OCD lesions (arthroscopy); and CT not only visualises the changes seen on using radiography, such as osteoarthritis and UAP, but also reveals the presence of incongruity and focal changes of the coronoid process.
KEY POINTS
- The canine elbow is a hinge joint made up of the humerus, radius and ulna.
- Developmental elbow disease is an umbrella term encompassing multiple developmental abnormalities of the elbow joint.
- Fragmented coronoid process is a common condition where the medial coronoid process of the ulna fissures and separates from the rest of the ulna.
- Osteochondrosis is a disruption of endochondral ossification resulting in abnormally thick layers of cartilage instead of subchondral bone. This can crack and fissure and form an osteochondritis dissecans lesion.
- Medial compartment disease is the extensive loss of cartilage and the collapse of elbow joint resulting from developmental elbow disease.
- Radiography can be a useful took in first opinion practice, however the two dimensional nature means not all pathology can be detected, therefore, a combination of computed tomography and arthroscopy is recommended to reliably identify elbow pathology.