Basic knowledge of the feline and canine ear canal is important. The external ear canal is similar in both species but there are subtle differences which can make investigation and management of disease different (Njaa et al, 2012).
External ear
The external ear canal is composed of the ear pinna and the external auditory meatus. There is a wide range in size and conformation of the canine ear pinna, ranging from the short prick ears of the terrier to the long pendulous ears of the spaniels.
The vertical canal is formed from the auricular cartilage which is rolled into a tube. The funnel-shaped vertical canal extends from the entrance down to the tympanic membrane. As it turns medially, it telescopes over the annular cartilage. The horizontal canal is composed of the annular cartilage and the proximal part of the auricular cartilage. The external ear canal in the dog is relatively longer than that in the cat and contains more hair. Some of the newer ‘designer’ breeds such as the cockapoo and labradoodle contain large amounts of hair in their ears which represents a challenge in treatment when they develop ear disease.
Middle ear
The middle ear separates the external acoustic meatus from the internal ear. The main structures within this area are the tympanic membrane; the tympanic cavity; the three auditory ossicles (malleus, incus and stapes); and the auditory tube. Although the basic structures are similar, differences do exist between the dog and cat.
Dog
The tympanic cavity in the dog is a thin-walled pear-shaped structure. It is contained within the petrous temporal bone and situated both caudally and medially to the temporomandibular joint. The tympanic membrane which separates the vertical canal from the tympanic cavity is a thin translucent membrane which is oval, and appears to be concave when viewed from the vertical ear canal. The tympanum is composed of the pars flaccida and the pars tensa. The manubrium of the malleus is attached to the dorsal aspect of the pars tensa.
Nerves that are in transit in relation to the middle ear are:
- The sympathetic post-ganglionic nerves to the eye and orbit from the nerve cell bodies located in the cranial cervical ganglion
- The facial nerves that branch from it — chorda tympani
- Branches of the glossopharyngeal.
Cat
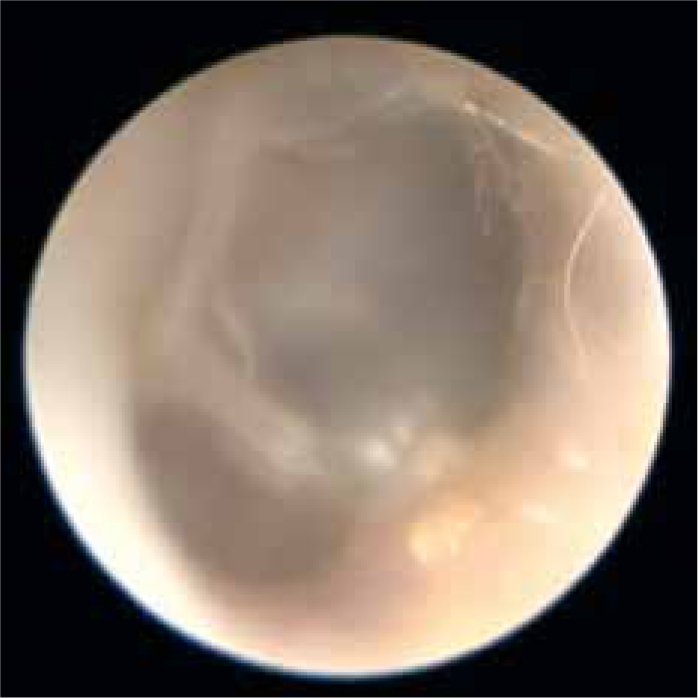
The tympanic membrane in the cat is similar to that in the dog, but has a slightly different shape of malleus to the dog (Figure 1). The tympanic cavity is divided into two chambers by a bony septum. The ventral cavity is much larger than the smaller rostrolateral cavity and the two communicate via a foramen at their medial aspect. The cat's tympanic cavity is otherwise very similar in structure to the canine tympanic cavity.
Infection in the external ear canal
Infection is always a secondary factor in otitis externa, and any investigation of ear disease should always include steps to identify and treat underlying primary causes. However, identification and therapy of infection is also important. Table 1 details the most common secondary infections seen in otitis in the ears of dogs and cats. Cytology is essential in all cases because it allows rational decision-making for investigation and therapy (Tater et al, 2003; Njaa et al, 2012). The appearance of the canal and type of discharge can also provide clues as to the type of infection that is present (Table 2).
Table 1. Most common bacterial and yeast infections identified from the ears of dogs and cats
| Secondary infection in otitis externa | |
|---|---|
| Bacteria | Acute disease: Gram-positive bacteria Staphylococcus spp., Streptococcus spp., Corynebacterium spp., Enterococcus spp. Chronic disease: Gram-negative bacteria Pseudomonas spp., Proteus spp., Escherichia coli |
| Yeast | Malassezia spp., Candida spp. |
Table 2. General appearance of the canal in each type of infection
| Infection | Appearance of the canal |
|---|---|
| Malassezia spp. | Canal swollen, erythematous usually pruritic. Thick dark brown ceruminous discharge. Often swelling of ceruminous glands to produce a cobble-stoned appearance |
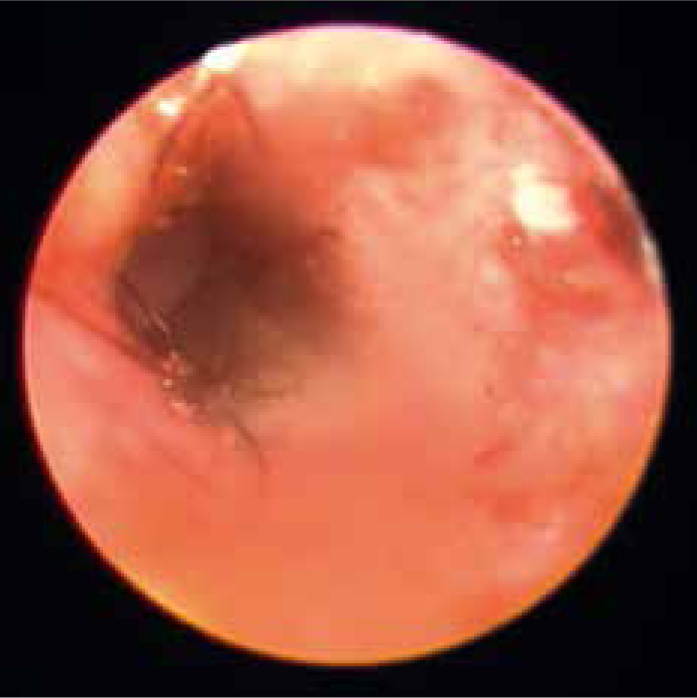
| Staphylococcus spp. | Canal swollen, erythematous often with ulceration. Usually painful rather than pruritic. Discharge yellow/pale brown ceruminopurulent (wax mixed with purulent exudate). Ceruminous gland hyperplasia uncommon (Figure 3) |
| Pseudomonas spp. | Canal swollen, severe ulceration and haemorrhage, very painful. Discharge malodorous green/yellow mucopurulent |
Cytology
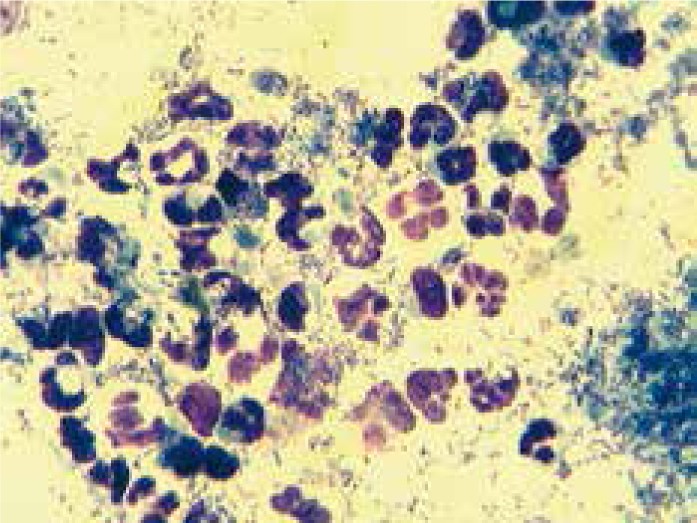
Cytology is an easy investigative technique and can be undertaken in the practice laboratory. Discharge may be collected from the ear using a cotton-tipped applicator rolled along a glass slide, heat-fixed and stained using Diff-Quik® stain. If peanut-shaped yeast or cocci bacteria are identified on cytology, therapy can be selected on an empirical basis. When rods are identified with a Diff-Quik stain, it is difficult to know if they are Gram-negative rods, e.g. Pseudomonas spp. or Gram-positive rods, e.g. Corynebacterium spp.. In these cases, cultures are important (Figure 2) (Tater et al, 2003).
Selection of therapy
In many cases, where for example only yeast is identified on cytology, therapy can be selected purely based on cytology. Ear cleaners should, in the opinion of the author, be used in all cases. Where there are large amounts of wax present, a cleaner with good ceruminolytic properties should be used. Components of ear cleaners that have good wax-removing properties include sodium docusate, squalene and carbamide peroxide. Potent ceruminolytics like carbamide peroxide should be used with care in the clinic and are best not dispensed to clients. Where there is a mixture of wax and purulent material in bacterial infection, especially with Staphylococcus spp., (Figure 3) ear cleaners should incorporate gentle ceruminolytic such as propylene glycol and antiseptics such as chlorhexidine and lactic acid. In cases of Pseudomonas spp., it is important that gentle ear cleaners are used. Astringent ear cleaners — those containing alcohol or those with a low pH — should be used with care if the ear canal is ulcerated. Products containing TrizEDTA™ products are useful in these types of infections (Harvey et al, 2014a).
Ear drops should be prescribed based on the type of glucocorticoid, antibiotic and antiyeast drug they contain. All ear drops contain anti-yeast components such as miconazole, clotrimazole, posaconazole, nystatin or terbinafine. Glucocorticoid potency varies between ear drops and should be considered when ear drops are chosen. When there is severe swelling and hyperplasia of the ear, a potent glucocorticoid such as mometasone or hydrocortisone aceponate is useful. Less potent glucocorticoids such as prednisolone may be adequate where the change to the canal is less marked. Antibiotic selection should also be carefully considered. Where possible, a narrow spectrum drug should be used. Fusidic acid and florfenicol represent good firstline drugs when Staphylococcus spp. is suspected. Fluoroquinolones should be reserved for the more severe infections with bacteria such as Pseudomonas spp. (Harvey et al, 2014b).