The North Island brown kiwi (Apteryx mantelli) (Figure 1) is one of New Zealand's endangered native birds. Kiwis live in forests and forage on the forest floors, they are unable to fly and have very little defence against predators such as rats, stoats or dogs, and this is the reason for their decline. Kiwis are classified as ratites, however, their large feet and inability to fly are really their only similarities to their larger relative the ostrich.

Kiwis also produce the largest egg in relation to their body size. The egg takes up 20% of the female's body; this is significant compared with an ostrich egg which takes up 2% of the female's body (Morgan, 2008).
At the Wellington Zoo there are five kiwis, two of these are part of a captive breeding programme.
Case report
‘Ataahua’ (Maori, meaning beauty) is a 4-year-old female North Island brown kiwi. She is Wellington Zoo's only female and is part of a captive breeding programme. She presented initially in late December 2009 as lethargic and was found in her burrow lying on her side collapsed.
The keepers brought her to the zoo's hospital where she was given a full examination, her abdomen was palpated and a blood sample was collected. The abdominal palpation revealed nothing unusual, and the blood sample was checked for any signs of an infection process by looking at the white blood cell count, which was only slightly elevated (Table 1). She was given 20 ml of saline orally via a soft crop tube. She was kept in hospital where her weight and behaviour were closely monitored. She was stabilized with daily fluids to ensure she could withstand a general anaesthesic for further diagnostics. After 2 days she was stable enough for radiographs, they were taken under general anaesthesia, using Isoflurane and oxygen administered via a long mask specially designed for kiwi beaks (Figure 2).
| Test | Result Dec 2009 | Result Feb 2010 | Reference range | Value |
|---|---|---|---|---|
| WBC(10^9/L) | 16 | 8.7–14.5 | ||
| HCT | 34 | 45.0 | % | |
| Glucose | 0.2 | 3.0–3.9 | mmol/L | |
| Uric acid | 79 | 300–380 | mmol/L | |
| Ca | 6.4 | 6.48 | 1.85–3.1 | mmol/L |
| Na | 106 | 138 | 140–178 | mmol/L |
| K | 3.7 | 12.2 | 3–3.6 | mmol/L |
| Na/K | 28.6 | 11.3 | ratio | |
| Cl | 80 | 103 | 110–142 | mmol/L |
| T protein | 76 | 26.0–110 | GM/L | |
| Albumin | 35 | 10.0–29.0 | GM/L | |
| Globulin | 41 | 16.0–33.0 | GM/L | |
| Alb/Glo | 0.854 | ratio | ||
| AST | 63 | 64–138 | U/L | |
| CPK | 506 | 521–971 | U/L | |
| A/G ratio | 0.9 | ratio | ||
| Bile acids | 1 | <35 | μmol/L | |
| GGT | 0 | 6.0–11.0 | U/L |
(reference ranges from Morgan, 2008)
WBC, white blood cells; HCT, haematocrit; T protein, total protein; Alb/Glo, albumen/globulin; AST, aspartate aminotransferase; CPK, creatine phosphokinase; A/G ratio, albumen/globulin ratio; GGT, gamma-glutamyl transferase

Lateral (Figure 3) and ventral dorsal radiographs were taken, as it is normal practise to take the two views to allow a better overview of the internal organs such as kidneys, liver and lungs. The radiographs indicated there was an apparent large soft tissue density mass in her abdomen; the mass was not clearly defined but was causing the other abdominal organs to be displaced and also reduced the definition of the organs.
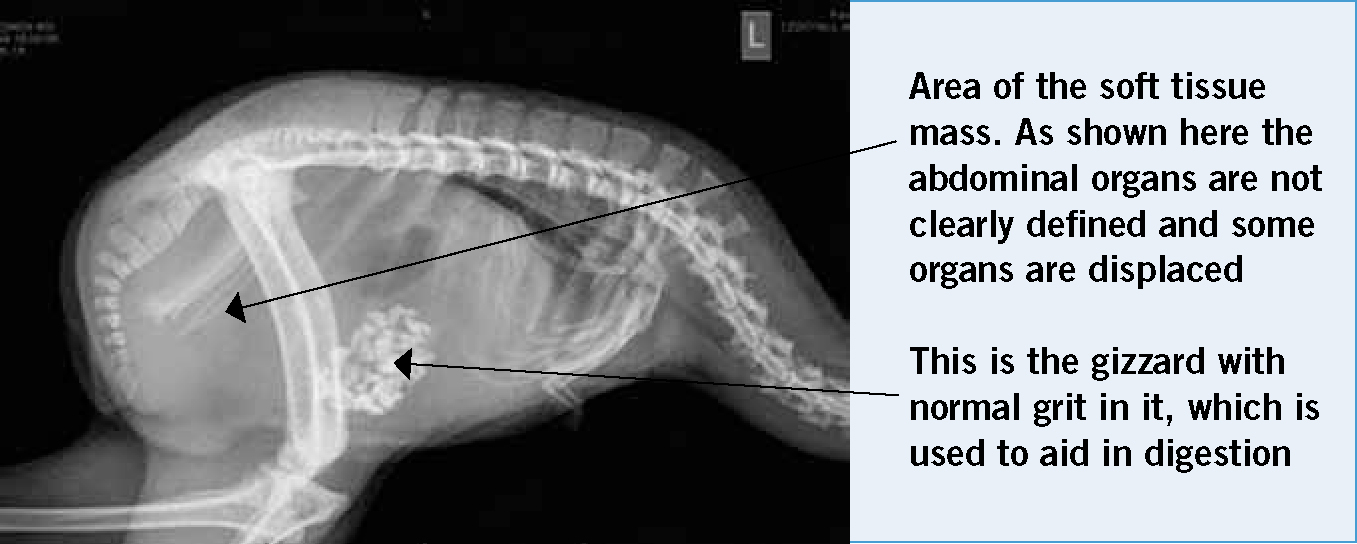
It was thought that the mass was most likely a recently ovulated, non-calcified egg within the reproductive tract and appeared to be passing normally. Blood results revealed an elevated calcium level (December 2009; (Table 1), which rises during egg formation, this combined with the soft tissue mass found on the radiographs led the zoo staff to the conclusion that Ataahua was forming an egg.
After analyzing all the results it was decided that the unusual behaviour of Ataahua lying on her side was caused by discomfort from the forming egg. She was maintaining her weight well and was demonstrating normal behaviours, such as foraging during the evening, which was recorded by the spread of faecal material through the enclosure. She was returned back to her enclosure where the keepers observed for any loss of appetite, weight loss or change in behaviour.
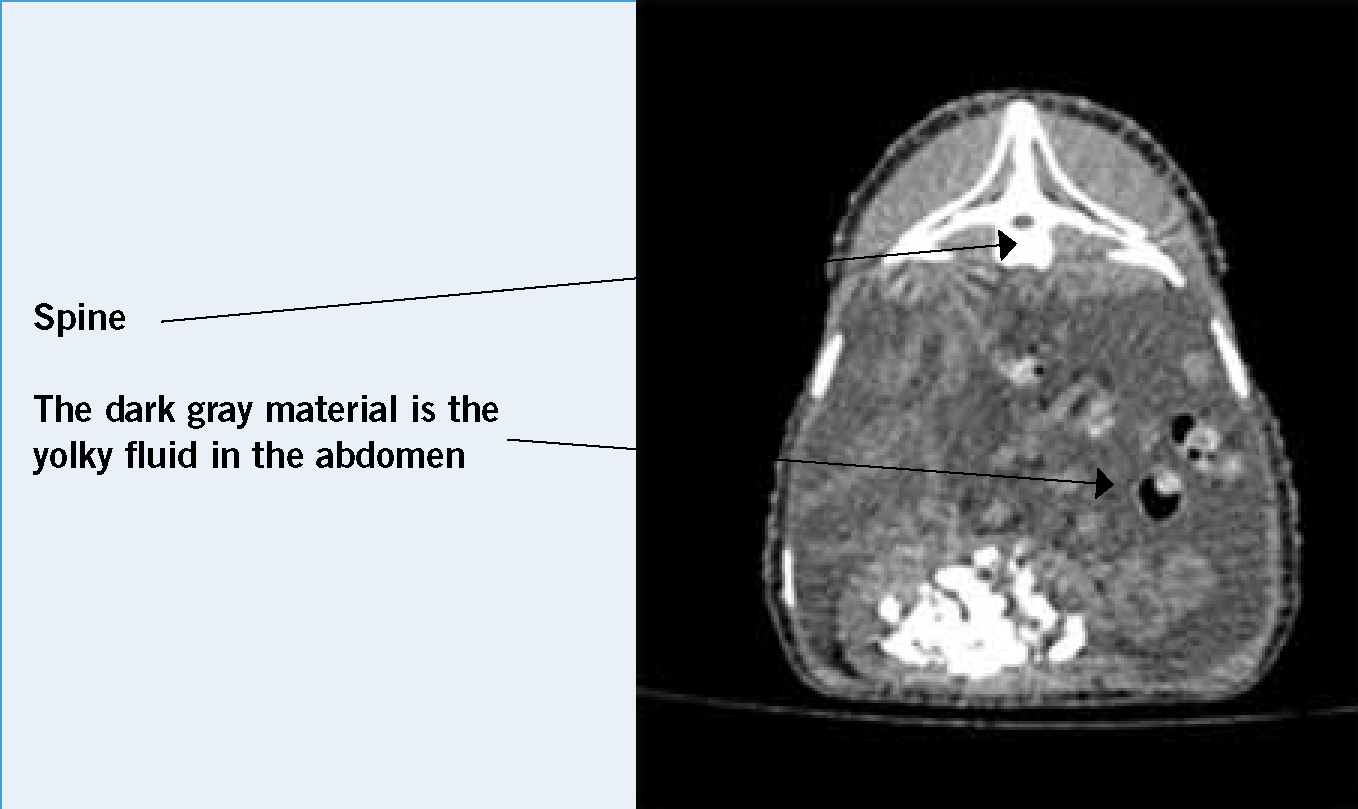
Ataahua had not produced the egg after 4 weeks, the normally timeframe is 5 to 7 days, so it was decided to perform a computed tomography (CT) scan. The advantage of this technique is that it provides increased definition and reveals more varied views of the organs. Ataahua was taken to Pacific Radiology, a human radiology facility in Wellington, where she was given general anaesthesia for the CT scan.
The CT scan revealed that there was an abnormal amount of fluid around the abdominal organs (Figure 4).
While she was anaesthetized abdominocentesis was performed and straw coloured fluid was retrieved from the abdomen. This was placed in sterile, plain and EDTA collection tubes and sent to a laboratory for cytology and culture. The cytology results of this fluid showed a small quantity of necrotic debris, which is possibly from the skin at the venipuncture site. Further blood samples were taken and the results are tabled below (February 2010; (Table 1).
The discovery of the fluid in the abdomen combined with the fact that the egg had not been passed and was no longer forming led to the diagnosis that Ataahua had egg yolk coelomitis. If left untreated the yolk can become septic causing septiceamia or as the body reabsorbs the yolk it can cause the organs in the coelomic cavity to adhere to one another.
It was decided that the best treatment for Ataahua was an exploratory laparotomy to remove as much yolk as possible and examine the reproductive tract for underlying disease. A laparotomy was performed under general anaesthetic (Figure 5) the following day. Ataahua was intubated with a non-cuffed size 3.5 mm endotracheal tube, and maintained on isoflurane and oxygen. An intravenous indwelling catheter was inserted into the lateral metatarsal vein, a solution giving set was attached, and 2.5% glucose solution was administered during the procedure at a fluid rate of 10 ml/kg/hr. The surgical site was prepared by plucking the feathers using non sterile haemostats and then washed with a solution of aqueous chlorhexidine. A heat pad underneath and an overhead heat lamp kept the patient warm during surgery. Avian veterinarians Kerri Morgan and Brett Gartrell from Massey University Wildlife Hospital performed the surgery. The surgery involved a ventral midline incision into the abdominal cavity, then removal of as much of the egg yolk from the abdomen as possible.

The abdomen was full of thick yellow yolky fluid with a small amount of blood and this was removed from the abdomen with sterile swabs. The reproductive tract was examined and showed no significant abnormalities and the abdomen was closed using absorbable suture material. Ataahua was left on oxygen until she was conscious enough to hold her head up, and then placed in a warm room overnight to recovery.
After surgery Ataahua was placed on antibiotics and anti-inflammatories. Although, the abnormal abdominal fluid was sterile, antibiotics were used to prevent infection after the coelomic cavity had been open for a long period of time during surgery. The anti-inflammatories were used to prevent organs adhering in the abdomen. Both drugs were given orally with a soft crop tube, and flushed with 10–20 ml saline. Ataahua had her surgical wound checked daily in hospital for 15 days, she was weighed to ensure she maintained weight and the food was also weighed to see how much she was eating. The extent of her night time activity was measured (by studying the spread of faeces through the enclosure and disturbance of leaf litter) to ensure that her nocturnal behaviours were not too disturbed. After the course of antibiotics was finished she was returned to her enclosure.
Discussion
Egg yolk coelomitis is also referred to as egg yolk peritonitis. Coelomitis is more accurate as birds have a coelomic cavity not a peritoneal cavity; these are differentiated by birds not having a diaphragm in contrast to mammals which do.
Egg yolk coelomitis can be caused by an ectopic ovulation, reproductive tract obstruction or impaction or if the oviduct ruptures (Lorenzo, 2003). In the case of the ectopic ovulation, this happens when the oviductal fimbrium fails to catch the ovulating follicle. It was suspected that an ectopic ovulation was the cause of Ataahua's disease, as there was no obvious disease of the reproductive tract.
When the laparotomy was performed, the reproductive tract was examined carefully making sure it was all intact, which it appeared to be. In some cases, if the reproductive tract is damaged or severely diseased a salpingohysterectomy (oviduct removal) can be performed to stop any further breeding, complications and reoccurrence of the disease. The ovaries are not normally removed in birds as they are so close to the kidneys, adrenals and aorta which makes removal too risky (Scott Echols, 2002). In kiwis, the removal of the uterus does not switch off the hormonal pathways which results in ovulation and these birds will continue to ovulate. If the reproductive tract has been removed they are susceptible to egg yolk coelomitis.
Further possible complications as a result of egg yolk coelomitis can include infection and adhesion formation (Crosta et al, 2003; Morgan, 2008). Although the yolk is initially sterile, it provides the perfect environment for bacteria to grow in and this results in septic coelomitis, which if left untreated could cause the bird to die. Normally the body reabsorbs the yolk and while this happens abdominal organs can adhere to one another, which may lead to the organ not being able to function normally if left untreated. The early stages of this were seen in Ataahua during the laparotomy and she was put on anti-inflammatory drugs to help prevent this occurring.
During surgery the abdomen was swabbed out with moist sterile swabs to remove the yolky material and also to prevent any adhering as discussed earlier. Alternatively the abdomen could have been flushed with sterile saline. This method is not commonly used in bird surgery because birds have air sacs in the abdomen and the flushing of fluids could cause them to drown. However, kiwis have smaller airsacs so the risk of this is greatly reduced.
Another complicating factor of laparotomy surgery, which is specific to birds, is a result of opening the abdominal air sacs. When opening the abdomen one inevitably opens air sacs. These are very thin walled structures and heal very well, but during the surgery this means some of the inhalational anaesthetic agents will escape from the open airsacs, making it difficult to maintain a nice plane of anaesthesia. With abdominal airsacs opened, the bird tends towards a lighter plane of anaesthesia. Consequently, when the surgeon closes the abdomen the bird can move to a deeper plane of anaesthesia as the respiratory tract becomes a closed system again. Other possible complications with anaesthetics include heat loss; as the central nervous system is depressed and unable to regulate temperature adequately, to avoid too much heat loss Ataahua was placed on a heat pad with a heat lamp over the top.
Conclusion
Ataahua was a very interesting case to be involved with as not only are these birds so special to New Zealand, but her case was also not straight forward from the beginning. Ataahua was saved by the amount of care that went into her treatment plan. She was given every possible treatment option and the outcome was successful. As it is planned that she will breed in the future any abnormal behaviours or weight loss will be kept closely monitored.
Although the disease is not common, there have been other findings of egg yolk coelomitis in kiwi throughout New Zealand (Morgan, 2008), unfortunately most cases of this disease are diagnosed post mortem. Therefore, with an understanding of egg yolk coelomitis and with prompt treatment more female kiwis like Ataahua could be saved.