There is increasing awareness within the veterinary profession of the importance of good management of post-operative pain (Slingsby and Waterman-Pearson, 1998; Morton et al 2005). Potential complications with the patient may arise if pain is uncontrolled. Uncontrolled pain may result in the animal becoming anorexic, or negative changes occurring to the patient's vital parameters, including negative behavioural changes (Logan, 2007).
Methods for evaluating pain post operatively in animals may prove to be difficult. The inability of patients to accurately express their feelings of pain or suffering increases the duty of care of those who undertake this responsibility. However, in spite of the difficulties veterinary clinicians should produce valid, reliable pain assessment tools for patients that are incapable of self reporting (Morton et al, 2005; Robertson, 2007).
Hellyer and Gaynor (1998) and Robertson (2007) have stated that pain should be thought of as the fourth vital sign, considered alongside temperature, pulse rate and respiration rate, in all patient evaluations. However, pain can only be recognized or measured with appropriate clinical examinations and the assessor being knowledgeable in pain recognition. Methods for scoring pain in animals have been restricted to the use of three subjective rating scales originally developed for human use: the simple descriptive scale (SDS); the numeric rating scale (NRS); and the visual analogue scale (VAS) (Morton et al, 2005). Other recognized pain scoring systems that may be used for pain scoring include the variable rating scale (VRS), dynamic and interactive visual assessment scale (DIVAS), Glasgow composite pain scale (GCPS) and the Melbourne pain scale (MPS). These have all been used successfully in veterinary practice. It has been suggested that these scales may simply be measures of how well the post-operative behaviour of dogs or cats fit the author's preconceived expectations for what constitutes pain-induced behaviour (Lascelles, 2004). This view is supported by Holton et al (1998) who believe that the scales mentioned are unreliable in the measurement of acute pain in dogs. Pain scoring systems should, however, still be an integral part of an animal's post-operative evaluation despite the problems that can occur with them (Robertson, 2007). Against this background of differing opinion on assessing pain this article reviews the literature on pain assessment and pain scoring post operatively in patients.
The importance of using a pain scoring model
There is growing interest by veterinary clinical specialists in exploring the nature of an animal's reaction to pain and how best to treat it (Hansen, 2003). Pain assessment research in animals has been conducted mainly to increase the understanding of the mechanical act of pain in reference to humans, however the recent growth in veterinary clinical studies have increased interest in pain assessment studies in animals, to their benefit. The majority of pain assessment scales were initially developed for humans and then adapted for animal use. This may be thought of as a barrier to creating the perfect pain scoring scale for animals (Carsten et al, 2008).
With this factor considered when assessing pain in animals, its measurement has been the subject of much debate in numerous pain scoring research articles (Bateson, 1991). However the need to measure pain has been acknowledged and a number of different methods have been used to assess pain in animals. The most commonly used methods rely on subjective observations of the animal's behaviour in the form of pain scoring scales (Holton et al, 1998). A human research study on verbal pain scores demonstrated an inadequacy and infrequency of analgesic administered to patients with painful conditions (Silka et al, 2004). The study concluded that using a pain scoring system improved analgesia administration patterns for trauma patients in the emergency department. This, however, was a verbal study and obviously could not be used in veterinary patients, but does highlight the importance of using pain scoring models and the positive outcome that can come from their use.
Physiological factors
Physiological factors may be considered a very important aspect in aiding pain assessment, including changes in heart rate, respiratory rate, pupil dilation, increases in body temperature and changes to the patient's blood pressure. The physiological factors mentioned are most commonly cited as indicators of pain in literature, however very little research has been undertaken to investigate the validity of these factors in pain assessment. A clinical research study came to the conclusion that findings of heart rate and respiratory rate were not useful indications of pain in hospitalized dogs (Holton et al, 1998). They also confirmed that pupil dilation would not be a useful tool in the assessment of pain. Physiological values when assessing pain have been found to be unreliable. However, it is thought that these would enhance pain assessment in some cases of pain recognition.
It has been suggested that with respect to pain assessment in animals simple observation is an inadequate method of appraisal (Lascelles et al, 1998). Most research regarding pain assessment in humans that are incapable of self reporting has been undertaken in neonates. The methods used rely on the changes in behaviour including a method of behavioural measurement.
Behaviour scoring is widely used in analgesic research with studies using the VAS system to assess analgesia requirements and sedation, therefore this method of pain assessment is the most commonly used scoring system for post-operative pain management in animals.
Pain scoring models
SDS
A study looking at chronic pain in humans indicated that a 10–20 point scale provided a sufficient level of information to describe pain intensity (Matthews, 2000). The most basic pain scoring system in veterinary medicine is the SDS. This scale usually has 3-5 grades of choice defined by a short description, for example, a pain score of zero would be ‘Happy, content, minimal body tension, confortable when resting, no reaction to palpation of wound on surgery site and interested or curious in surroundings’ (www.burnsurvivorsttw.org/articles/painass2.html). It is easy to use, however, the negatives include the huge variation seen between assessors when scoring animals and the lack of sensitivity, with assessors able to ‘jump’ from one number to another without detecting small changes in the patient's pain intensity (Grant, 2006). Waterman-Pearson (1999), however, believes that a SDS is a useful way to assess pain as it combines visual appraisal, interaction with the patient and palpation of the painful area, incorporating multifactoral pain scoring systems.
NRS
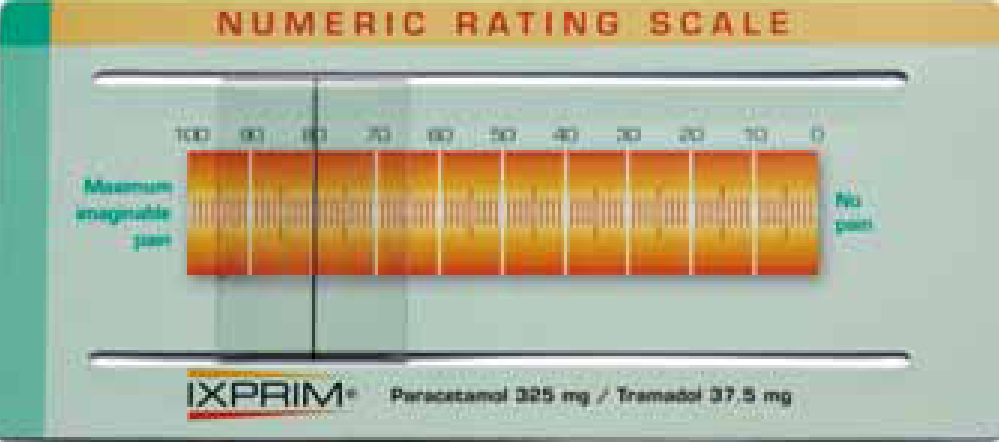
The NRS is very similar to the VAS (see below), however, the observer assesses the patient and then chooses a rating of pain based on a scale of 0–10 or 0–100 rather than using a mark on a line (Figure 1) (Grant, 2006). The NRS is commonly chosen in practice as it has been used extensively in the measurement of pain in human medicine. It has been suggested that it takes the adequate middle ground between the lack of sensitivity of the SDS and the difficulty of using the VAS (Holton et al, 1998). The NRS is one of the most commonly used methods of scoring pain that is based on subjective observation of an animal's behaviour (Holton et al, 1998). Morton et al (2005) applied a scaling model to establish and validate an interval level pain scale in the assessment of acute pain in dogs; a NRS was used as one of the methods and it was found that it was advantageous as it takes an animal's behaviour into consideration during the pain assessment. However, it is thought that the behaviour aspect of an animal's pain may well be affected by sedation or recovery from general anaesthesia and this should be taken into consideration when pain is assessed.
VAS
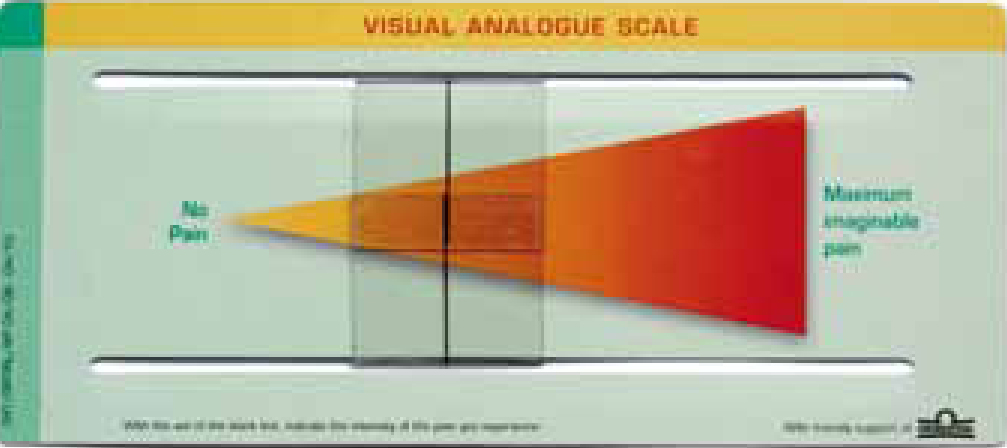
The VAS is a 100 mm line with one end representing ‘no pain’, and the other end representing ‘the worst possible pain’ (Figure 2). It has been criticized for being influenced by the visual and motor co-ordination of the observer, which reduces the ability of users to accurately place a mark on the line (Holton et al, 1998). Some believe that the VAS may allow for over interpretation, however, users would require training and experience in the successful use of VAS (Tranqulli et al, 2004; Grant, 2006). Stanway et al (2002) explained that all pain scoring is performed by an observer and difficulties with placing the mark on the VAS line were unlikely to be a problem; the problem could be overcome by allowing the operator to become familiar with the scoring system prior to the start of the assessment.
Previous work on pain scales in human and veterinary studies have shown the VAS of assessment to be useful but the ability to differentiate easily between relatively small variations in pain have been demonstrated.
VRS
A VRS may also be used in assessing pain post operatively, however research literature discussing this method of assessing pain is scarce. The VRS incorporates physiological data collection, including heart rate, respiratory rate, pupil size and rectal temperature, when assessing for pain, as well as the patient's behaviour. This system is considered a sensitive and reliable method of pain assessment despite different assessors using the system (Grant, 2006). A number is chosen from the scale dependant on the definition or description of pain being experienced by the patient. These numbers provide an overall total score once the pain assessment is complete.
DIVAS
DIVAS may be described as a modified VAS that incorporates an interactive dynamic assessment. The patient is first observed undisturbed, then assessed on being approached, handled, during palpation and while walking. Similar to the VAS a mark is then made on a 100 mm line. Grant (Grant, 2006) has explained that pain may proceed undetected if purely observation with no interaction is used to assess a patient in pain. Because of this the DIVAS is generally considered inherently more sensitive than the SDS.
Animals may have a low pain score when visual observation is used alone (Shih et al, 2008). The animal's discomfort may not be detected until an assessor performs the second phase of the pain score, which includes interaction, and the third phase (III), which includes palpation. The DIVAS III measurement is always higher than DIVAS I. This research emphasizes the importance of interacting with the patient for a complete assessment to ensure that pain experienced by animals does not go unnoticed (Shih et al, 2008).
GCPS
The GCPS is another method for the assessment of acute pain in animals (Grant, 2006). It is based on the McGill pain questionnaire used in humans and consists of six sections that include assessment of different behavioural aspects of animals. This includes assessing any vocalization of the patient, whether there is any attention to the painful area, the motility of the patient, response to palpation and touch, demeanour and the patient's posture within the kennel area. The GCPS is currently the only scale validated for use in the assessment of acute pain in dogs. It is believed to be a reliable clinical tool for defining different pain intensities and a change in pain score over time in dogs undergoing a variety of surgical procedures (Murrell et al, 2008). However, Valtolina et al (2009) have suggested that it can be particularly difficult to assess pain in dogs that are critically ill because systemic disease may obtund normal behavioural signs of pain. See www.gla.ac.uk/faculties/vet/smallanimalhospital/ourservices/painmanagementandacupuncture to download a GCPS form.
MPS
The MPS is very similar to the GCPS in that it involves observations in several categories with a score for each category, both behavioural and physiological assessments are considered. The MPS has been referred to as an effort to improve on the simplicity of the VAS scoring system (Hansen, 2003). When the MPS was applied to dogs following ovariohysterectomy it showed good agreement between different users (Grant, 2006), leading to the conclusion that it looked very promising for use in future clinical practice. It has been suggested, however, that if the MPS was applied to dogs post surgery they would be assigned a low pain score because the scale would not capture the correct information (Hansen, 2003). For example, in post limb amputation the dog may lie quietly, be unwilling to move, fail to eat and appear very depressed. A total score of four out of 27 may have been recorded for this particular patient. See http://dels-old.nas. edu/ilar_n/ilarjournal/44_3/v4403hansen.pdf for an example of the MPS.
Pain assessment
There are numerous methods of assessing pain in animals, however, the assessor should be aware of and familiar with the signs of acute pain and how it affects an animal's behaviour. It is essential for veterinary surgeons and veterinary nurses to be confident at interpreting signs and symptoms of pain in patients (Flaherty and MacGillivray, 2003). There is very little information regarding assessing pain without the use of pain scoring systems. Pain scoring systems can be useful in tracking the animal's response to any analgesia that has been administered (Flecknell, 1994).
Consequences of pain
Ongoing pain may lead to a variety of problems including an increased risk of infection, delayed wound healing, a reduction in voluntary eating and water intake, mobility problems, altered sleeping pattern and a change in normal behaviour. The detrimental effects of unrelieved pain may also affect the cardiovascular system, respiratory system, gastrointestinal system, urinary system, metabolism, nervous system and immune system (Grant, 2006). Unrelieved pain can even result in increased morbidity and mortality in patients (Grant, 2006).
Protocol
Any pain assessment protocol should include the assessor becoming familiar with the patient's normal and presenting physiological values, including their behaviour before the pain response is initiated if possible. This would provide a baseline.
Recommendations for veterinary practice
The author recommends that good pain management is a part of every patient's rehabilitation post operatively in veterinary practice. This would ensure that the patient is assessed regularly and that the need for additional analgesia was noted. It has also been suggested within the literature (Grant, 2006) that the future of pain assessment and pain scoring models would appear to be a multidimensional approach. Included in this multidimensional approach are the behavioural assessment of the patient and the physiological assessment of the patient. A strong practice commitment dedicated to minimizing pain and assessing pain at a high standard would have to be implemented. Ideally the veterinary staff should be trained in the use of the pain model and staff training would include all staff responsible for observing patients on a daily basis including animal nursing assistants.
It has been establwished that the assessor must be familiar with the patients presenting physiological values (temperature, pulse and respiration) and behaviour. A thorough pain assessment should ideally include both non-interactive and interactive evaluation of the patient (Figure 3) (Grant, 2006). It is also recommended by the author that a series of assessments should be performed by the same person at regular intervals, and analgesia administered as directed by the veterinary surgeon. All of these recommendations must be performed with the use of a common pain scoring system that is sensitive to small variations in pain intensity. When selecting a pain scoring model the physical status of the patient must also be considered. It would be inappropriate to select a pain scoring model that assesses the patient's mobility if the patient was recumbent.

Recommendations for further study
The literature review has highlighted that further investigations are required in the field of successful pain management and pain scoring systems. It is also recommended that the investigations concentrate on comparison of different pain scoring models when assessing pain in patients. This would highlight recommendations for the most accurate pain scoring system for use in veterinary practice. The majority of the literature reviewed focused on pain scoring systems that aim to assess the efficacy of certain analgesia protocols rather than make direct comparisons between currently used pain scales.
The investigations would help to produce a universal pain scoring protocol for veterinary practices that could subsequently benefit post-surgical patients with the common goal of excellent pain management included in the aftercare of patients.
An ideal pain scale for animals is one that not only detects the presence or absence of pain but can also measure the magnitude of its severity, its location, and how it makes the patients feel (Grant, 2006). A review of the most common methods for assessing pain in animals post operatively indicates that the ideal pain scale does not exist. However, aspects of behavioural and physiological assessment of patients may be used in conjunction with a scoring system to enhance pain recognition. Daily pain scoring with an acceptable pain scale should be used when managing pain, and this can only improve patient pain management (Carsten et al, 2008).
Ongoing reminders of the focused intervention of pain management were shown to improve care in a human emergency department (Silka et al, 2003). This study concluded that standardized pain assessment would improve pain management in patients.
Stanway et al (2002) included sedation in their preliminary investigation as the level of consciousness in a patient was thought to affect the assessment of pain. The importance of the sensitivity of pain scoring systems has also been questioned. When researchers used a VAS and NRS scoring system they failed to detect differences with a placebo group (Slingsby and Waterman-Pearson, 2000). This may suggest that the VAS and NRS are not sensitive enough to detect small variations in levels of pain. Further research would help to determine this.
It has been suggested that patients should be assessed as individuals (Shih et al, 2008) and that knowledge of the patient's behaviour when assessing pain before treatment can be very helpful when assessing them post operatively. Again, it would be interesting to research this further.
Conclusion
Pain assessment of patients post-operatively may be enhanced when the normal behaviour of a patient is known and physiological factors are also considered. This information should, however, be used in conjunction with a pain scoring system that is sensitive and familiar to the observer, and assessment should be performed at regular intervals to ensure the adequacy of the analgesia is determined. If all these factors are considered when assessing pain in patients post operatively excellent pain management can be achieved.