

Many procedures we carry out in veterinary practice are complicated and depend on a series of steps being carried out correctly to be effective. We are all human and it is very easy to miss out one small step, which can lead to an error.
These errors are more likely to occur if we are stressed, distracted by other things going on, rushing, tired or hungry. Other factors that contribute to errors identified by Oxtoby et al (2015) are lack of communication, teams that are understaffed or do not work well together, a poor practice culture or lack of systems of work.
One system of work that may help to reduce errors is a checklist. Checklists are lists of vital actions which need to be completed before, during, or after a procedure by compensating for the limits of our memory, they can act as a trigger to remind us of crucial steps that are easily overlooked. They improve team communication, and consistency and quality of care. They have been proven to reduce complications and errors in many safety critical industries such as in aviation and human medicine (Thomassen et al, 2014).
Checklists can reduce patient harm and improve consistency of care in veterinary practice too (Bergstrom et al, 2016), and are one of the many tools we can use as part of a framework within our practice for continuous quality improvement.
Quality improvement and clinical governance
Clinical governance is a requirement of the Royal College of Veterinary Surgeons (RCVS) Code of Professional Conduct for veterinary nurses (RCVS 2012). Scally and Donaldson (1998) defined clinical governance as ‘a framework through which organisations are accountable for continually improving the quality of their services and safeguarding high standards of clinical care by creating an environment in which excellence in clinical care will flourish’. Clinical governance sets out what registered veterinary surgeons and veterinary nurses must do.
Quality improvement (QI) is ‘the combined and unceasing efforts of everyone to make the changes that will lead to better patient outcomes, better system performance and better professional development’ (Batalden and Davidoff, 2007). QI tells us how to carry out clinical governance, and other continuous improvements, by using recognised tools to identify gaps, analyse data and test changes.
In the veterinary world, QI should involve the whole practice team in looking at areas that could be improved to provide better care for our patients, better outcomes and a safe learning culture in practice.
By completing audits we can generate data which allows us to understand:
- The success rates of our care (known as outcome audits)
- The impact of the way we provide care (process audit)
- Whether we have the right kit or facilities available to provide the care that we provide (structure audit)
- What is going wrong, or exceedingly well, and why (significant event reports and significant event audits). When we have the data available, we can compare our results to other care providers, whether that be other veterinary surgeons, veterinary nurses, other branches in the group, other practices or all practices on a national level (known as benchmarking).
The point of QI is that once we understand the level of care we provide, we should then implement interventions to try to improve it. As well as responding to the needs of any structural audits, common QI tools are checklists, guidelines and protocols. These should all be designed using evidence-based theory, and with modern approaches to leadership. Whenever an intervention is introduced, it is important to carry out audits to check if they are being used as intended (process audits) and to check whether the changes have resulted in improved outcomes (outcome audits).
If we are benchmarking and sharing our results, we can learn from each other, for the benefit of the animals in our care, we can understand more safely and quickly if there are better ways to do things.
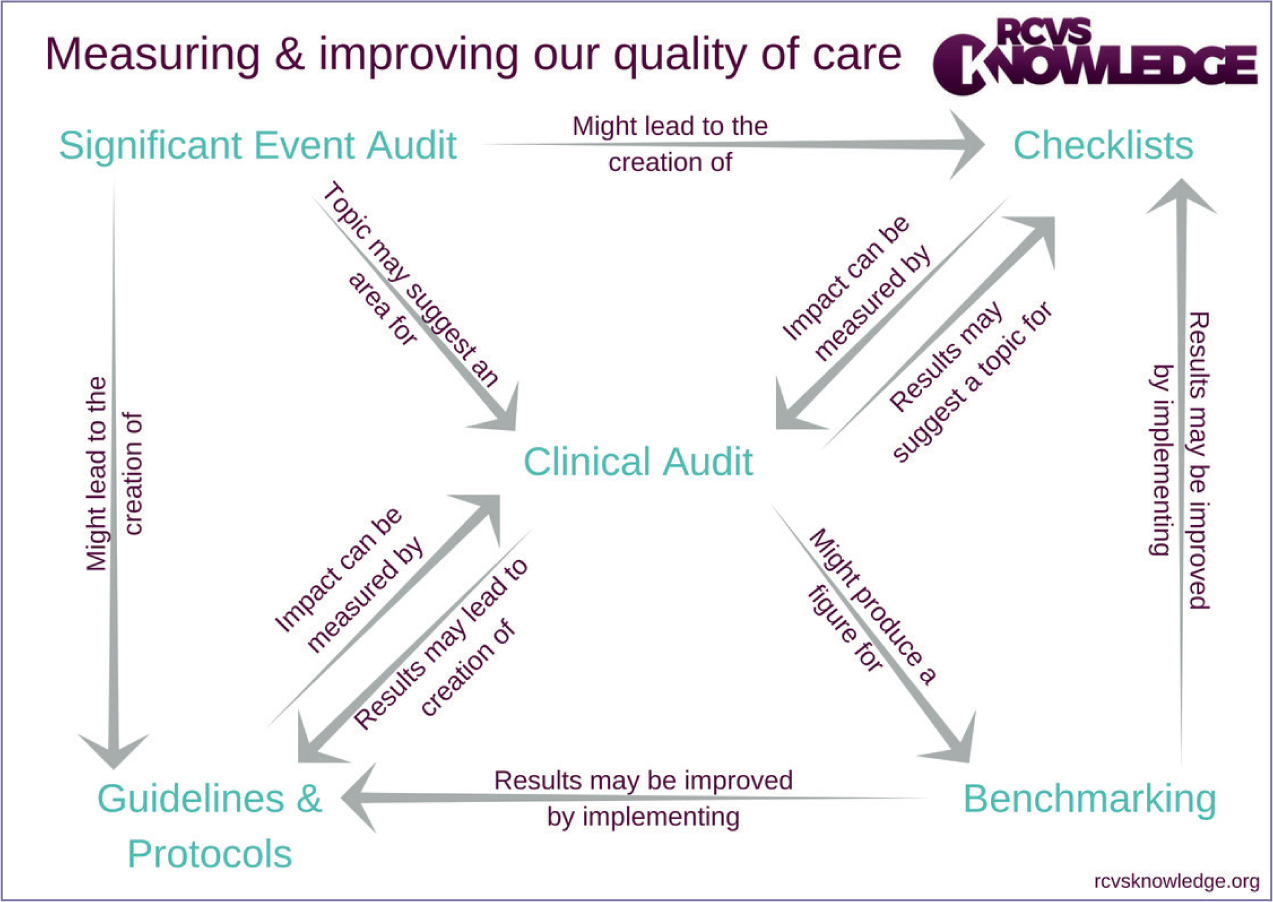
Checklists are an important system of work, one of the QI tools practices can use along with other systems. These activities link together to form a strategy for practices to embed a culture of safety and continuous quality improvement in practice (Figure 1).
Resources to assist with all these processes can be found at: https://knowledge.rcvs.org.uk/quality-improvement/tools-and-resources
Checklists in other industries
Checklists have been used in aviation since the 1980s. Pilots do not solely rely on memory when undertaking procedures in the plane or if there are mid-air issues. In aviation they recognise that human factors, such as stress or tiredness, can increase the likelihood of error and can affect performance (Sexton, 2000), so they have a checklist for every eventuality which is read out by one of the pilots while the other pilot works through the steps. This is a ‘read do’ checklist (or they may sometimes use a ‘read confirm’ checklist). Both are important communication tools used between pilots. Checklists are unique to each type of aircraft and are constantly updated following modifications to the plane, or through lessons learned through accidents or near misses.
In 2001, Peter Provonost, professor at Johns Hopkins University School of Medicine, devised the first checklist for human medicine. He made a list of all the steps required to avoid central line associated infections:
- Wash hands
- Clean skin with chlorhexidine
- Sterile drapes on patient
- Wear mask, hat, gown and gloves
- Put a sterile dressing over site when done.
Central line infections at that time were involved in 30 000 to 62 000 deaths annually in the USA.
He carried out an audit before introducing the checklist and found that 30% of time, at least one step was not followed. He then introduced the checklist and authorised nurses to stop doctors if the checklist was not followed. Infections were reduced from 11 to 0% (Laurance, 2009).
Then, in 2008, the World Health Organisation (WHO) introduced a surgical safety checklist in an effort to improve safety during surgical procedures and reduce adverse events (Figure 2). Atul Gawande was involved in this project which he describes in detail in his book The Checklist Manifesto. This checklist is designed to accompany patients from the start of anaesthesia to recovery. The crucial stages for patient safety are: before induction of anaesthesia; before skin incision; and after the procedure.
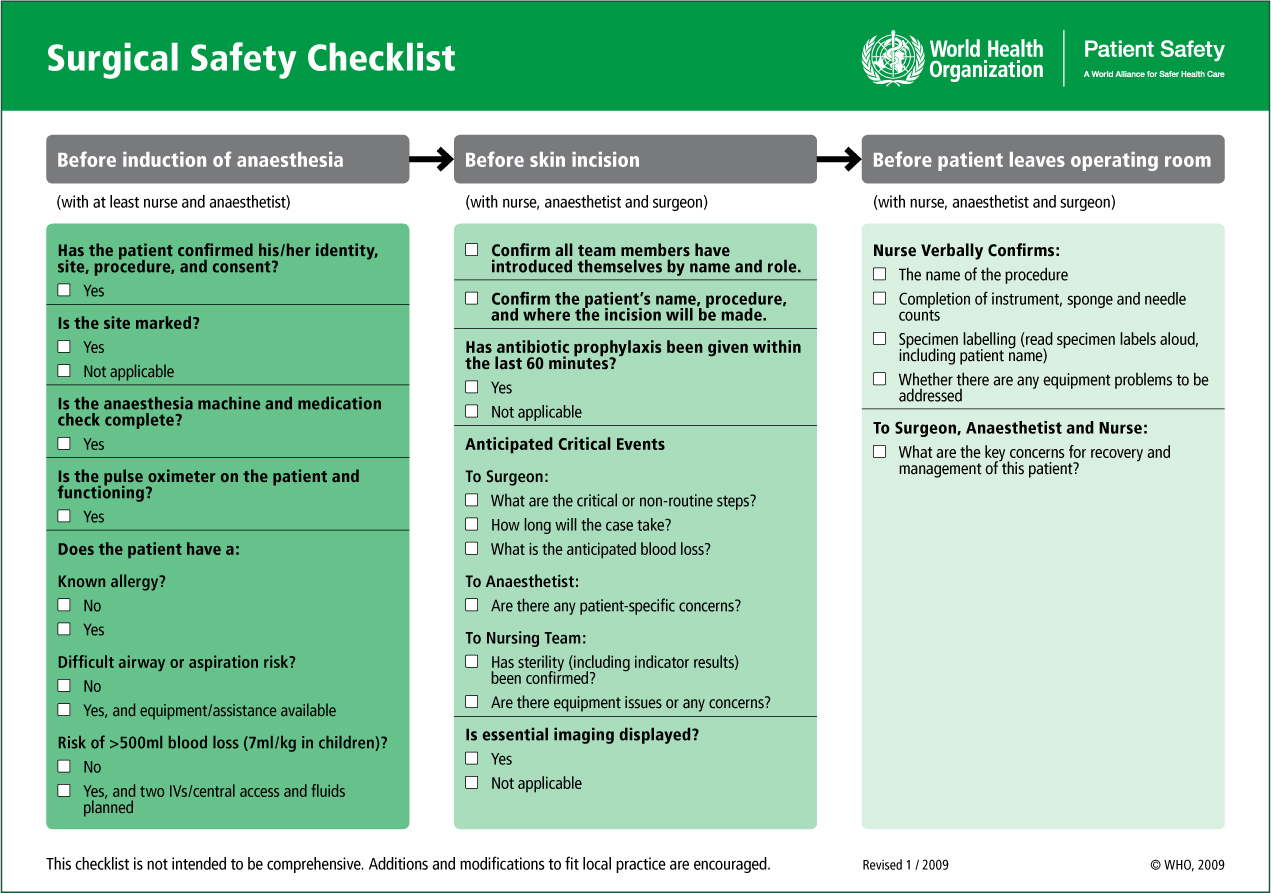
Before induction of anaesthesia — sign in
The important points to check at this stage are that we have the correct patient, the correct procedure, the correct site. That the patient has no known allergies. Whether there are any specific safety concerns for anaesthesia. To ascertain whether all of the anaesthetic equipment has been checked.
Before skin incision — time out
Here it is suggested that team members introduce themselves and their role. This may not be as appropriate in small teams who work together constantly (although, even in these cases, this step has the potential to mark out more formally the roles and responsibilities of each team member). This stage gives an opportunity to discuss any anticipated safety concerns for the procedure by the surgeon and the anaesthetist, and for the nursing team to confirm that all required instruments are available and sterile.
After procedure — sign out
This is the stage when instruments and swabs are counted and any samples are clearly labelled. It is also important here to discuss postoperative monitoring and care.
Results of using a surgical safety checklist
At these three main points the team stops and the appropriate stage of the checklist is read aloud. Provided all is confirmed, the procedure continues.
A version of this checklist is used for all surgery in the NHS and in many hospitals worldwide. It has been proved to reduce errors, injuries and death. The results of the pilot study in 2009 are shown in Table 1.
Table 1. In the pilot study in 2009
| Deaths fell 47% |
| Complications fell 36% |
| Infections fell 48% |
| 78% of team members said it had prevented an error |
| 93% of team members said they would want it to be used if they were the patient undergoing a procedure |
Using a surgical safety checklist should also reduce the incidence of ‘never events’. Never events are serious incidents that are wholly preventable because safety systems are available and should be used. This applies to areas such as wrong site surgery, retained swabs or instruments, which should be able to be prevented by use of a checklist (Burnet et al, 2014).
Checklists in veterinary practice
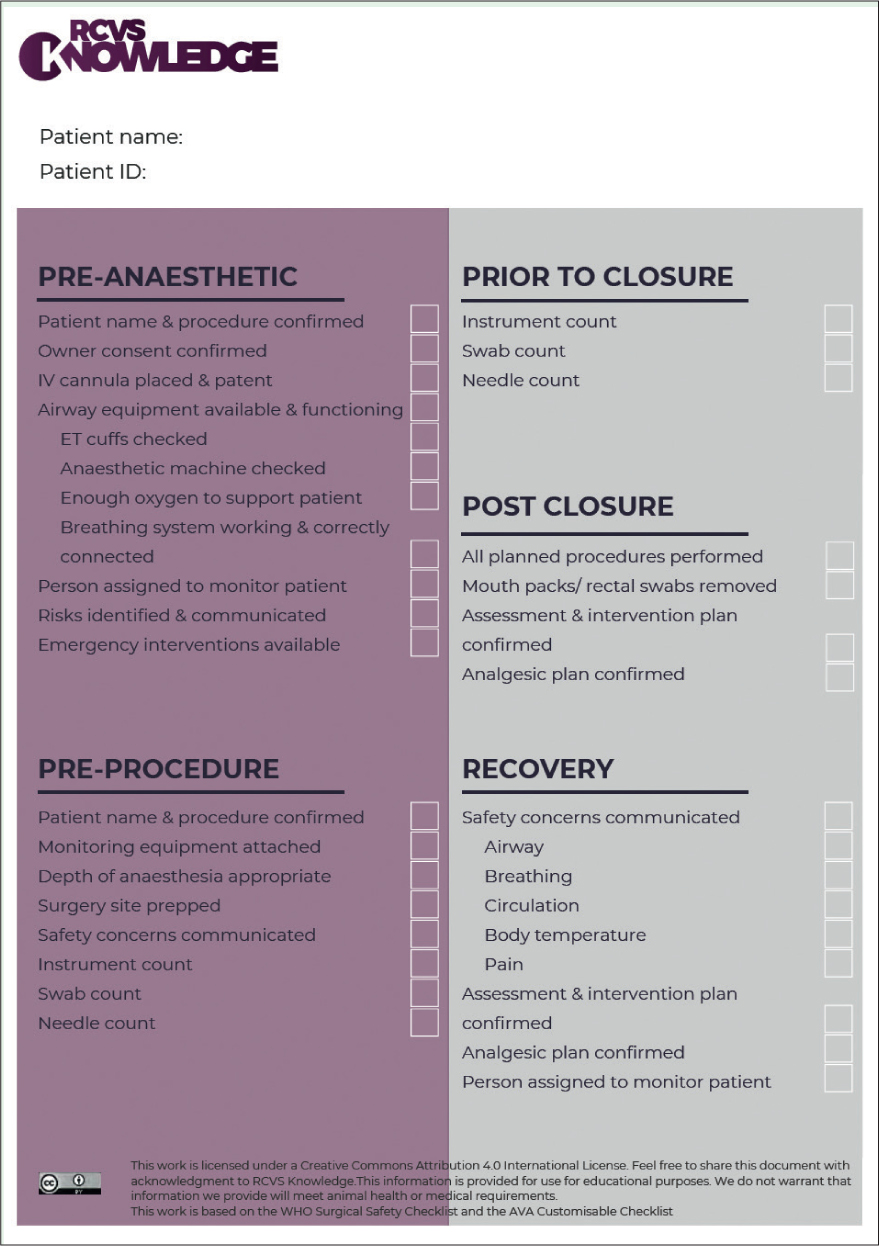
Many veterinary practices are now using modified versions of the WHO Surgical Safety Checklist. There are multiple examples from a range of practice settings as set out in the Royal College of Veterinary Surgeons (RCVS) Knowledge Surgical Safety Checklist Manual (Figures 3 and 4). www.rcvsknowledge.org/document-library/surgical-safety-checklist-manual/
Bergstrom et al (2016) found that the frequency and severity of post-operative complications was significantly decreased after introduction of a surgical checklist in veterinary practices. Thomassen et al (2014) found that surgical safety checklists strengthened compliance with guidelines, improved human factors, reduced the incidence of adverse effects and decreased morbidity and mortality.
Implementation of checklists
Before implementing a checklist it is a good idea to audit your current level of care so any improvement following use of the checklist can be measured, for example, before implementing a surgical safety checklist you could audit postoperative complications of surgery.
Redpath and White (2018) found acceptance and adoption of a surgical safety checklist in an equine hospital was poor. The main barrier is often that the team do not see the benefit of the checklist. As with all QI projects, if they are not introduced properly or the team are not on board from the start, they are less likely to be successful. Involving the team from the start allows everyone to have some ownership for the improvement process. They are then given the chance to understand why changes are being implemented, to ask questions and to be involved in its design.
It is important to overcome perceived barriers that it will be time consuming, necessary for some but not others, that it would be difficult to implement because of perceived or existing hierarchy, or that it reduces clinical freedom.
The checklist should be personalised to the needs of that particular practice, rather than using a one size fits all approach.
It should not be too long or too complex. The ideal checklist should be short (less than 10 items), simple, evidence-based, and in clear large type. If too many checklists are introduced at once, teams may experience ‘checklist overload’.
Time must be allocated for team training around the checklist and appointing a ‘checklist champion’ can help to get the team on board and ensure consistent use. The team members reading out the checklist questions should be empowered to stop the procedure if the checklist is not used. It also helps if practice leaders engage with the checklist from the start and use it consistently.
Putting these steps in action, and promoting an honest learning culture, will give the practice a much better chance at introducing a checklist that will be used.
After a short period of using the checklist, use a process audit to see if the checklist is being used as and when it should be, and an outcome audit to see if it is having the desired effect — sometimes the changes made will not be the right ones or might need some tweaking. There should be a feedback session for team members and, if necessary, the checklist can be modified. Any barriers to its use should be identified with changes made to the checklist as a result.
The WHO has a very useful surgical safety implementation tool that can help with implementing a checklist: https://www.who.int/patientsafety/safesurgery/checklist_implementation/en/
Not just a piece of paper
A checklist is a communication tool. It does not need to be filled in to be effective, as long as the team work through the actions on the list. Checklists do not need to be read out, but there is evidence that if someone speaks during a procedure (reading out the checklist for example), they are more likely to speak up if they experience any issues (WHO, 2020).
Checklists encourage non-technical skills, including situational awareness, teamwork, decision making and good communication (Armitage Chan, 2014). This is illustrated in Figure 5.
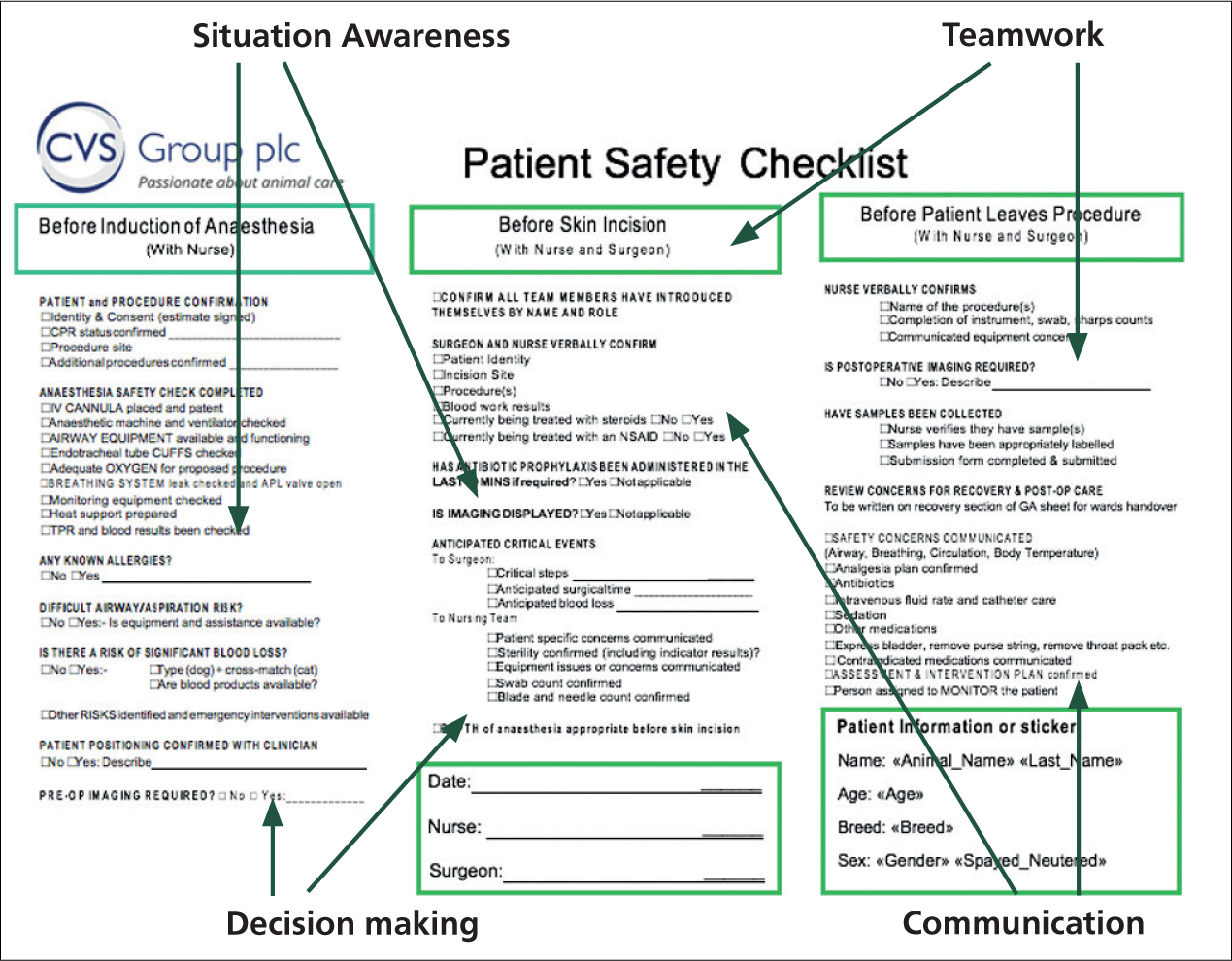
For checklists to be really effective, practices need a culture of teamwork, clinical leadership and assertiveness in raising issues.
Other areas where checklists are useful
The Association of Veterinary Anaesthetists (AVA) have produced a very useful anaesthetic checklist and an implementation manual: https://ava.eu.com/wp-content/uploads/2015/11/AVA-Anaesthetic-Safety-Checklist-FINAL-UK-WEB-copy-2.pdf (Figure 6).
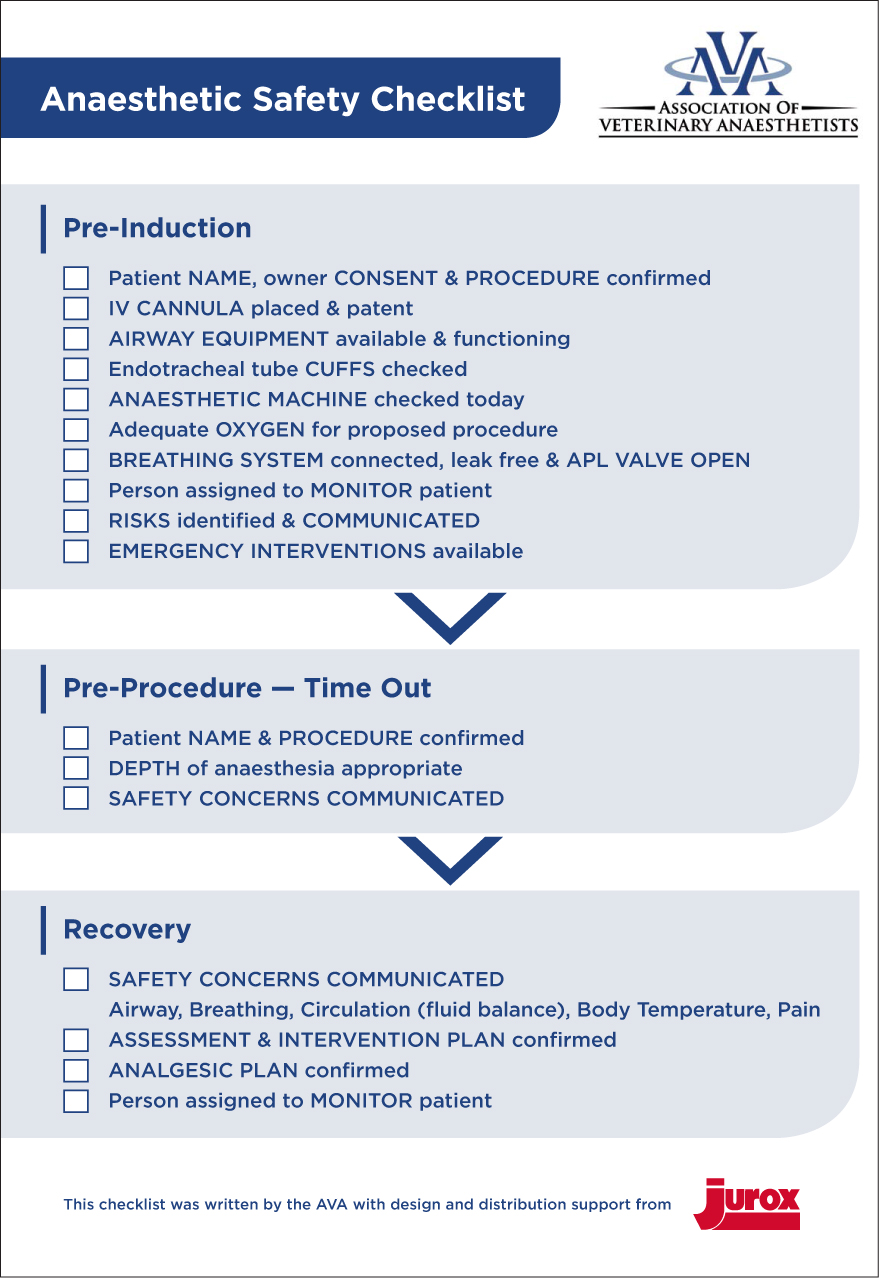
Anaesthetic checklists on hand held devices can also be combined with dose calculator apps to help to reduce errors. Checklists are also extremely useful in case handover situations to ensure all relevant information is captured when shifts change. This is another area when team members may be tired and rushing so making errors more likely to occur.
Other areas where checklists can be useful include checklists of required equipment for specific surgeries, triage checklists and cleaning checklists.
Patient safety systems
Checklists are one of the systems we can put in place to try to reduce errors. Others include guidelines and protocols, team training and continuing professional development (CPD), technology solutions, workflow design, work environment, equipment design and packaging and labelling design.
Using a systems approach to improving patient safety allows problems to be addressed not by trying to modify human behaviour, but by modifying systems instead by analysing risks. It is not about trying to eliminate human error, but rather about designing systems that make errors less likely to occur and to cope with errors that do occur. It is about looking at how the whole practice works, rather than focusing on what individuals are doing.
When things go wrong, it is most often because of system design flaws rather than failures of people. Errors are not usually caused by ‘bad people’, but due to ‘bad systems’, or a lack of a system altogether.
The practice dispensary can be the source of many errors and near misses, but it is also a place where systems can really help. There should be robust protocols and team training in place, but physical systems can also help. Examples can vary from medicine packaging, designed to clearly identify different sizes and designed so as to not resemble other medicines, to storage arrangements whereby dangerous fluids that might be mistaken for others are kept in different locations (or are marked with red tape, for example), to fully automated dispensaries where a medicine name is typed and only the section with the relevant medication opens.
Human factors
Workplace planning should encompass human factors, with workplaces designed to make it easier to do the right thing and harder to do the wrong thing. Involving practice team members who know how work is actually carried out in planning systems of work is always useful, as they have insights into how the work is actually done rather than how management may imagine the work is done.
Having standardised equipment throughout the practice also helps, for instance, errors can be reduced if all syringe drivers throughout the practice are the same and are calibrated in the same way. A good example of this can be seen on RCVS Knowledge's website — significant event audit case example: fentanyl CRI overdose. www.rcvsknowledge.org/document-library/significant-event-audit-case-study-fentanyl-cri-overdose/
Conclusion
In veterinary practice we cannot ever completely prevent errors. As humans, we are fallible, and in high-pressure environments, our capacity for memory recall is reduced further. But errors can be reduced by having systems of work in place, such as checklists. This will make work places safer and less stressful for our team members with better outcomes for our patients.
For further free examples and advice on how to get started with checklists and other quality improvement techniques, visit www.rcvsknowledge.org/quality-improvement.
KEY POINTS
- Checklists can compensate for limits of human memory.
- They are a system of work that can reduce errors.
- It is important to involve the whole team in introducing checklists.
- To be effective checklists should be modified following team feedback.
- The systems approach to safety is about designing systems of work that make errors less likely to happen.