
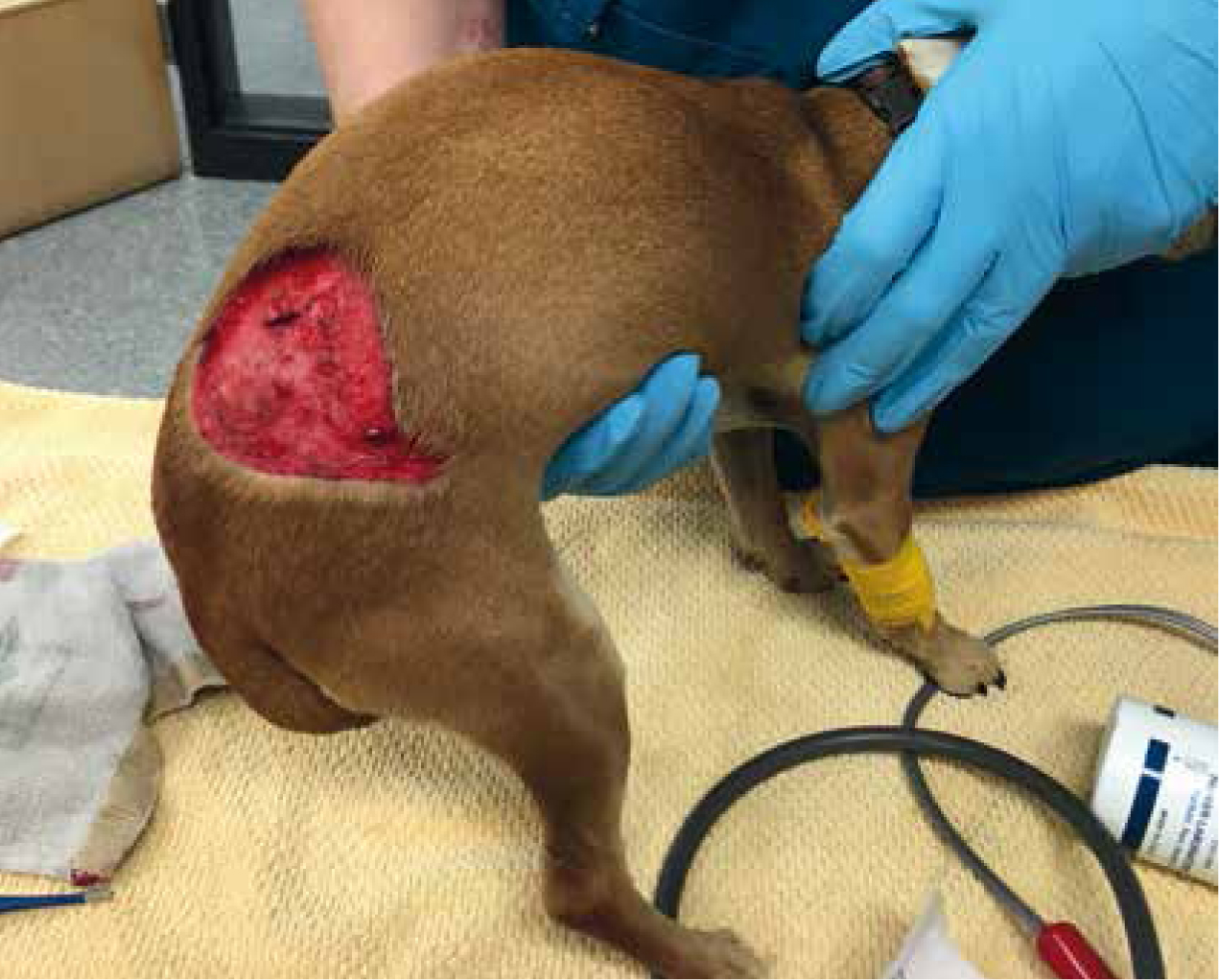
Wounds are a common occurrence in veterinary patients and trauma can often result in large and complex wounds which take specialised care to heal (Figure 1). While these more complex wounds take time, effort, and finances to heal, the reward at seeing patients heal makes treating these wounds worth the effort. The nursing team plays a vital role in patient care, bandage and patient management, and client education and must be familiar with how to treat a variety of wounds. There are a variety of wound types and treatment will vary based on the type. Wounds can be organised into the following categories:
When a patient presents to the hospital with a wound, regardless of cause or duration, the nursing team must be sure first to evaluate the entire patient starting with the patient's ABCs:
Traumatic situations leading to external wounds can also cause internal bleeding, lung injury, organ trauma, head trauma, and excessive bleeding that can lead to hypovolaemic shock. As blood and fluid loss and tissue damage occurs, perfusion to tissues and major organs will decrease. Reduced perfusion means decreased oxygen delivery to peripheral tissues and eventually to major organs. Shock occurs when cells cannot produce necessary energy due to the reduced oxygen delivery. Patients experiencing trauma can be in shock from lung injury (not performing gas exchange well enough to provide oxygen to cells), crushing injury (blood vessels are damaged and cannot carry oxygen to tissues) or from blood/fluid loss (not enough volume to carry oxygen to tissues). The clinical signs seen in these patients are the result of the body attempting to compensate for the lack of oxygen delivery and must be recognised so that treatment can begin immediately (Lichtenberger, 2011a).
In hypovolaemic shock, poor venous return leads to peripheral vasoconstriction, increased cardiac contractility, and an increased heart rate. With the resulting increase in cardiac output, the body is attempting to continue to bring normal blood flow to vital organs. Blood flow is restricted to the skin, extremities, and intestines first which will cause poor peripheral pulses, decreased blood pressure, pale mucous membranes, and increased CRT. As shock continues without treatment, the liver and kidneys receive reduced blood flow which can lead to organ dysfunction. As blood flow to the brain is not maintained this will result in a depressed mentation.
Heart rate, mucous membrane colour and CRT, blood pressure and body temperature must be measured on patient presentation, and any abnormalities addressed. Patients that present with these physiologic signs of shock need immediate treatment. Unless the patient has cardiac disease, the mainstay of shock treatment is intravenous fluid therapy. A large bore short length intravenous (IV) catheter will deliver a significant amount of fluids quickly and is ideally placed in a cephalic vein, as perfusion to the saphenous veins is compromised in severe shock. Crystalloid fluids are electrolyte and water replacement (Hartmanns Solution, Normosol-R, 0.9%NaCl for example) and are administered quickly in an attempt to restore circulating volume and therefore oxygen delivery to cells. The shock dose of crystalloid fluids is 90 ml/kg for a dog and 45 to 60 ml/kg for a cat. This dose is divided into smaller amounts (20 ml/kg for example) and administered as a quick bolus (Lichtenberger, 2011b) (Figure 2). Once the bolus is complete, the patient's vital signs are once again assessed. The bolus amount may be repeated until vital signs begin to improve. Baseline laboratory values such as packed cell volume and total protein levels, kidney function, blood glucose, and lactate levels can help in the overall patient assessment and can also help with anaesthetic planning.

Initial care of wounds
During the patient evaluation and initial treatment period, wounds can be coated with a water soluble lubricant to keep tissues moist and covered with a sterile non-stick pad and light bandage wrap to prevent further contamination (Monnet, 2011). If wounds are excessively bleeding, the bleeding must be addressed as part of the initial patient evaluation. Direct pressure can be applied to slow bleeding and temporary pressure bandages placed as needed. In severe bleeding, an inflated blood pressure cuff applied proximal to the wound and then inflated can slow bleeding. Alternatively, a tourniquet can be applied for a short period (15–20 minutes), but can cause severe tissue damage and tissue death if left in place for too long (Garzotto, 2009). Nurses should pay close attention to thoracic and abdominal wounds as some of these wounds may penetrate into the thoracic or peritoneal cavity. If a wound penetrates into the thoracic cavity, this will create a loss of negative pressure within the thorax, and the lungs cannot expand. These wounds must be covered immediately, and thoracocentesis performed to stabilise the patient for further treatment (Liss, 2012). Wounds thought to penetrate the abdominal cavity should be covered and care taken during wound repair so as not to contaminate the wound further.
Pain management
Pain management is a vital step in wound management and healing. Pain must be addressed early in the process for both patient comfort and to aid the healing process. Pain can lead to tachycardia, panting and decreased tidal volume, hypertension, and behavioural changes. Pain is often associated with sympathetic nervous system stimulation as a stress response and can lead to a decreased immune response, hypercoagulability, and vasoconstriction (Perkowski, 2009). Animals in pain often do not eat or rest as they usually would which can significantly impede healing. Pain must be addressed at the time of admission to the hospital and continually assessed during the healing process. Nurses can implement pain scoring scales in the hospital setting to standardise pain assessment and look for positive or negative trends in patients. Pain and patient response to pain should be discussed in nursing rounds to ensure continuity of care and continuous evaluation of pain. Owners must be instructed to watch for signs of increased pain such as decreased appetite at home, hiding, shaking, and licking/chewing at wounds. If owners are educated and encouraged to communicate with the veterinary team, patients are kept comfortable throughout the healing process.
Prior to wound closure
Before definitive wound closure or care, the veterinary team must perform a thorough assessment of the wound and develop a plan for healing. Every veterinary team member must wear gloves when dealing with wounds. Open wounds are susceptible to bacteria present on hands and in the hospital, but veterinary employees must also protect themselves from bacteria present in dirty wounds. In some traumatic accidents, human blood can be present on veterinary patients, and the veterinary team must employ basic safety measures. Significant wounds can require months of bandage changes, multiple surgical procedures, intensive care both in the hospital and at home for the patient, and a significant financial contribution from the client. Pet owners must be made aware of this commitment both emotional and financial as early in the treatment process as possible. The nature of wounds can change over time and owners must be kept apprised of these changes as time continues. The veterinary team should make a short and long-term cost estimate for owners and update this estimate as needed to ensure compliance and the success of healing (Tobias, 2012).
Wound cleansing
If a wound is deemed repairable (good blood supply to the wound, no infection present, and sufficient skin is present to close over the wound), the next step is to prepare the wound for closure. Nurses can protect exposed tissue with sterile, water-based lubricant and then clip the hair around a wide area surrounding the wound (Figure 3). The lubricant will keep the tissues moist as well as prevent hair, and other contaminants from sticking to the tissues. Clipper blades should be at minimum clean (potentially gas sterilised) and sharp so that further tissue damage does not occur during this step. While clipping, note any other wounds, bruising, or areas of necrosis immediately surrounding the wound. The skin surrounding the wound should then be cleaned with a 0.05% chlorhexidine or 1% povidone iodine scrub, using care not to scrub over the actual wound (Garzotto, 2009). Use chlorhexidine with care as concentrations greater than 0.05% are toxic to cells. Wound lavage is then performed to wash gross contamination from the wound. In heavily contaminated wounds, tap water from the faucet can be used and then sterile lavage performed after. Sterile lavage is best performed using a 35 cc syringe and 18 g needle to direct fluids to the wound surface (Figure 4). A 3-way stopcock, fluid administration set, syringe, and needle or intravenous (IV) catheter can be connected directly to a litre of lavage fluid for ease of lavage. Large quantities of lavage solution are required to fully wash debris from the wound. Commercial 0.9% saline solution is a common choice for lavage solution but is an acidic solution (pH 5.5) which may be detrimental to fibroblasts. Hartmann's solution and lactated Ringer's solution are less acidic than 0.9% saline (pH 6.5) and therefore can also be utilised as a wound flush (Buffa, 1997). For visibly infected wounds obtaining a culture before bandaging or closure may be warranted to help guide antibiotic therapy.


Once the patient has been assessed and treated for any shock, pain, and concurrent medical emergencies, further steps to wound care such as debridement, closure, and bandaging may require deep sedation or general anaesthesia. The goal is to make the patient the best anaesthetic candidate possible which means definitive wound treatment may need to wait until the patient's vital signs are stable. The nursing team must closely monitor vital signs, assess patient comfort, and monitor wounds for any changes until the animal is stable enough for further treatment.
Overall patient care
With any patient dealing with a large wound, care of the overall health of the patient is vital to proper healing. Maintaining adequate hydration is necessary to allow adequate perfusion to wounds. The veterinary nursing team must be comfortable assessing hydration and be vigilant to changes in patient status. Trauma patients with large or extensive wounds require nutrition to heal. Early intervention with feeding tubes is vital in hospitalised patients, and consultation with the owner regarding proper nutrition at home may be necessary for long-term wound management in some patients. Pain and stress can lead to vasoconstriction and must be avoided if at all possible to promote healing. Veterinary nurses are vital to keeping patients comfortable and stress free. With proper emergency care, good cleaning and lavage technique, appropriate bandaging and bandage management, and client education and compliance, patients presenting with traumatic wounds can return to an active, healthy life (Liss 2012).
Conclusions
In conclusion, the veterinary team must ensure a whole patient examination with every wounded patient to ensure acceptable airway, breathing, and circulation is present prior to addressing wounds. Pain management is essential to proper wound healing and must be tailored to the patient and the stage of healing
Veterinary nurses must properly clip, clean, and lavage wounds prior to debridement and bandaging. To optimise wound healing, whole patient care, including nutrition, must be monitored during the entire healing process.