

There is a global obesity epidemic in companion animals (Kipperman and German, 2018). Canine obesity (commonly defined as a body weight of 15% greater than optimal (Courcier et al, 2010)) is a significant health issue for companion pets. It is considered the most common form of malnutrition and is a common medical disorder in companion animals (German, 2010).
Large numbers of companion dogs are now classed as overweight or obese (German, 2006; Courcier et al., 2010). A recent retrospective study of a large sample size (n=24 247) by Gates et al (2019) has shown that canine obesity affects 28.4% of companion dogs in New Zealand, with similar rates found internationally (Courcier et al, 2010).
The implications of canine obesity on animal health are multiple and various, with obese dogs more prone to heart health concerns, diabetes, and joint injury and damage (Such and German, 2015; Gates et al, 2019). Obesity becomes a significant welfare concern because of its potential to decrease longevity (Courcier et al, 2011) and its negative impact on quality of life (German et al, 2012). With pet ownership in New Zealand being among the highest in the world (with 64% of households having at least one pet) (New Zealand Companion Animal Council Inc., 2016), the number of obese pets in New Zealand is significant. By comparison, US pet ownership is 67% (The Humane Society International of the United States, 2019) and UK pet ownership is 50% (PDSA, 2020).
The most widely recognised method to easily assess welfare is through the use of the ‘Five Freedoms’, a set of five guidelines that detail the necessities of life, including the provision of adequate food and water, shelter, disease prevention and treatment, as well as a lack of distress and the ability to perform normal behaviours (Manteca et al, 2012). When reviewing these in the context of canine obesity, it is reasonable to argue that some of the ‘Five Freedoms’ are not being met. To illustrate, overweight or obese animals are not free from malnutrition, because of a diet being fed in excess (Sandøe et al, 2016). Obese dogs are not free from pain, discomfort, and distress, with obesity known to cause or exacerbate health issues such as joint pain (Sandøe et al, 2016); and medical care may not be appropriately or promptly sought, or medical advice may not be being adhered to. In addition, dogs classed as obese may not be getting appropriate opportunities for exercise, which is considered a mandatory normal behaviour for dogs.
An accurate, repeatable, and cost-effective assessment of body composition is vital to ensuring accurate and consistent nutritional advice to pet owners. As such, veterinary medicine utilises body condition scoring as one method to help categorise under and overweight animals. Body condition scoring is a visual assessment of the degree of obesity in animals, with body condition score measures available for a variety of species (Ferguson et al, 1994; Vieira et al, 2015). Several systems are available, with a 9-point scoring system, developed in 1997 (Laflamme, 1997), being the most widely accepted (German et al, 2006) and recommended by the Association for Pet Obesity Prevention (Association for Pet Obesity Prevention, 2019) and the World Small Animal Veterinary Association (WSAVA) (Freeman et al, 2011). These body condition scoring tools provide a visual guide, often accompanied by a short description for each of the 1–9 points on the chart. Figure 1 shows the 9-point body condition score tool provided by WSAVA.

The WSAVA, along with the Global Nutrition Committee developed Nutritional Assessment Guidelines in 2011 (Freeman et al, 2011). A nutritional assessment of veterinary patients, of which bodyweight, body condition score, and muscle condition score are a part, is deemed so important that is has become one of the vital assessments of animal health, along with temperature, pulse, respiration, and pain (Chandler, 2010). A body condition score is one of the main ways of assessing obesity and is part of the nutritional assessment recommended by WSAVA as one of the five vital signs. Having this information allows for accurate education of owners regarding their pet's nutrition and exercise. Veterinary professionals can then use this tool along with clinical judgement from palpation of the animal to determine its body condition score, and thus its degree of variance from normal weight. While this visual tool is cost-effective, as no additional equipment or testing is required, it is still subjective and prone to errors because of the wide-ranging morphology of different dog breeds (Laflamme, 1997).
Body condition scoring is a technique that is quick and easy to apply to all canine patients entering a veterinary clinic and should be routinely undertaken within the veterinary practice by veterinary nurses prior to an animal's consultation with the veterinarian. While this tool does make it simple to body condition score a large range of animals, the varying morphology between different breeds means the chart is one-size-fits-most and not one-size-fits-all. Unfortunately, there is no perfect tool that will work for every dog, every breed, every time, but clinical judgement, whether that be from a veterinarian or qualified allied veterinary professional (veterinary nurse, veterinary technician, etc.) should always be an accompanying factor.
While body condition scoring is still a subjective assessment, as it is the opinion of one practitioner at one point in time, data relating to inter-observer reliability between various veterinary healthcare team members are scant with no recent studies determining the consistency between various clinical staff providing a body condition score. Without these data, it is difficult to know whether this presents an issue regarding accurately determining overweight and obese canine patients, especially if it is not the same person assessing the patient at every visit.
Owner understanding of their own pet's body composition is poor, with many underestimating the body condition score of their pets (scoring pets lower than they should be) and owners of overweight dogs normalising their obesity, even when presented with the tools to assess body condition score using a validated method (Eastland-Jones et al, 2014). Eastland-Jones et al (2014) found that 89% (63/71) of dog owners involved in the study underestimated their dog's body condition score (when compared with the study investigator's score), even when using a body condition score chart to aid them. Of the owners who did not use the chart to aid them, 92% (66/72) were underestimating their dog's body condition. Owners of overweight dogs were most commonly incorrect in their dog's body condition score. Additional studies have shown similar results, with Courcier et al (2011) finding that 53% of owners with over-weight dogs underestimated their dog's weight.
Discrepancies between veterinarian and owner perceptions of weight do occur and verbal discussions around pet nutrition and weight may not be sufficient (White et al, 2011). It is vital that veterinary nurses are not only providing clients with information on their pet's body condition score, but that this information is accurate. Specific verbal and written information on the animal's current weight status and weight management recommendations should be provided.
Critically important to the discussions around canine obesity is whether veterinary staff are providing suitable and timely advice to their clients around their overweight or obese pets. We already know that owners misperceive their pet's body condition, underestimating body condition score of overweight or obese dogs (Eastland-Jones et al, 2014). There is currently a paucity of data reviewing whether different veterinary nurses are making the same assessments of a body condition score on a patient and whether their assessments are influenced by their geographical area (urban versus rural), and potentially the morphology of the dogs they are more frequently seeing in practice.
The aim of this study was to investigate differences in the body condition score assigned to a canine (via photograph) by rural, city and suburban veterinary nurses with particular interest in whether the geographical area of the respondents' current veterinary practice influenced the score given to animals. It was hypothesised that city and suburban veterinary nurses would score dogs lower (more normal) than rural nurses, thereby normalising obesity in companion dogs, possibly because rural veterinary nurses are more exposed to working dogs, that have a higher tendency to be normal or lean weight, rather than obese (McGreevy et al, 2005). To account for possible experience of the veterinary nurse, the study also recorded the childhood geographical area of each respondent and whether it influenced the body condition scores provided.
Methods
This quantitative study used a cross-sectional design comprising 26 questions. A questionnaire targeting veterinary nurses in clinical practice in New Zealand was distributed via social media (private Facebook pages and via the New Zealand Veterinary Nursing Association (NZVNA) Facebook page) and email, to investigate the differences in body condition score assigned to canines (via photographs) by veterinary nurses working in city, suburban, and rural settings in New Zealand. This research was approved by the University of Glasgow College of Medical, Veterinary and Life Sciences Ethics Committee (Project 200190072).
Emails were sent to New Zealand registered veterinary clinics inviting veterinary nurses to participate in the study. Email addresses were obtained from publicly available information online. This sampling method relied on a degree of both convenience and ‘snowball’ sampling as participants were asked to share the survey among their peers and colleagues via their social networks. Follow-up reminders were distributed via Facebook, but not via email. As the questionnaire included screening questions to eliminate anyone from the non-intended audience, sharing of the questionnaire with non-veterinary nurses was not a concern. The questionnaire employed a mixture of open (not covered in this article) and closed questions. Questions related to demographic information (including age, gender, level of highest qualification, years working as a veterinary nurse), the type of clinic, geographical area of their current workplace (city, suburban or rural) and geographical area of the predominant area of their childhood. This final variable was explored as the predominant geographical area of their childhood may have been different from the geographical area of the current workplace, and as such may have been a confounding factor in the body condition scores assigned by an individual. Urban-city, Urban-suburban and rural were not defined for respondents, however the Oxford Dictionary provides these definitions: rural — in, relating to, or characteristic of the countryside rather than the town; suburban — of or characteristic of a suburb; city — a large town. Respondents would likely also be familiar with the rural/urban delineation from completion of New Zealand Census surveys. Respondents were also asked to assign a body condition score on a range of photographic images of dogs with a variety of different body conditions (ranging from underweight to obese), and answer questions relating to the body condition scoring of canine patients in their veterinary clinical settings (this section is not covered in this article and is intended to be published separately). Participants were asked to provide a body condition score using a 9-point scale, however no example scale or specific information on how to use the scale was provided. The images used in the study were selected by the researcher from images readily available on the internet and used under ‘fair use’ purposes for research. They were chosen as they represented a range of various body condition scores and included some images which would be deemed to be at the extreme of either end of the scale (based on the primary researcher's clinical judgement).
The research was conducted via an online survey utilising the survey tool OnlineSurveys.co.uk. The survey was designed to take less than 10 minutes to complete, and data were collected over a 2-month period in early 2020. Survey completion was anonymous, with no IP data obtained.
Data were analysed for descriptive statistics. Continuous data including age and years as a veterinary nurse were normality tested using the Shapiro-Wilk test revealing non-normal distribution, therefore results are described as median and range. Inferential statistics were performed using the Kruskal-Wallis test to determine if geographical location of workplace or predominant geographical area of their childhood had any impact on the scores assigned. This non-parametric statistical test was selected as the body condition scores data are ordinal and as such are not normally distributed. Results were considered significant if the p-value was ≤0.05.
Results
Results from 80 participants were obtained during the study period of 21 January, 2020 to 20 March, 2020. Of these, 77 responses were able to be used for data analysis as three respondents were veterinary nursing students. These 77 responses represent 3.5% (77/2145) of the New Zealand veterinary nursing population (Statistics NZ, n.d.).
Females comprised 100% of participants. The median age was 31 years, with a range of 20–62 years. A quarter (24.7%; n=19) of participants held a certificate level qualification, 62.4% (n=48) held a diploma level qualification, and 12.9% (n=10) held a degree level qualification.
Most veterinary nurses surveyed (75.0%, n=58) had been working as a veterinary nurse for less than 10 years, and most respondents (71.4%, n=55) worked in urban (city and suburban) areas (see Table 1 for full description of all demographic data).
| Age (n=77) | |
|---|---|
| Median, years | 31 |
| Range, years | 20–62 |
| Gender (n=77) | n (%) |
| Male | 0 |
| Female | 77 (100%) |
| Highest level of qualification | n (%) |
| Certificate level | 19 (24.7%) |
| Diploma level | 48 (62.4%) |
| Degree level | 10 (12.9%) |
| Years as a veterinary nurse | |
| Median | 6 |
| Range, years | 1–27 |
| Location of current workplace | n (%) |
| Rural | 22 (28.6%) |
| Urban-city | 22 (28.6%) |
| Urban-suburban | 33 (42.8%) |
| Location of childhood | n (%) |
| Rural | 32 (41.6%) |
| Urban-city | 11 (14.3%) |
| Urban-suburban | 34 (44.1%) |
| Clinic type | n (%) |
| Companion animal | 51 (66.2%) |
| Equine | 0 |
| Large animal | 0 |
| Mixed | 26 (33.8%) |
Box plots were used to visually determine which variables showed a difference between the three geographical areas (rural, suburban, and city) for current geographical area of the veterinary nurse's workplace (Figure 2).
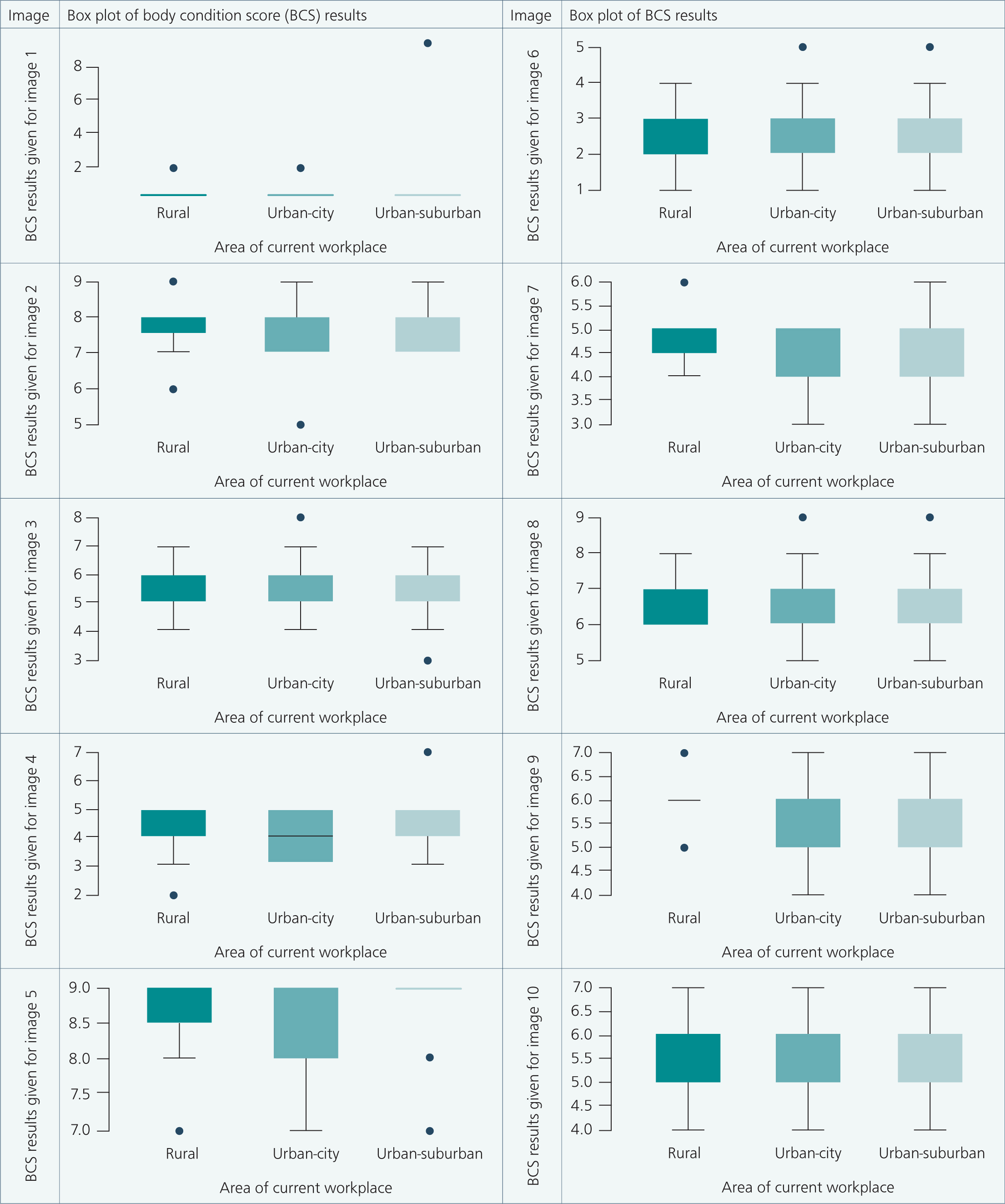
These variables were then further analysed using a Kruskal-Wallis test. None of the images showed any significance in result, with all p-values returned being greater than 0.05 (p-value range of 0.13–0.97). The same method was employed to evaluate any difference in image score when compared with the geographical area in which the veterinary nurse spent their childhood. No significant difference was found (p-value range of 0.17–0.99) between the scores given for veterinary nurses brought up in city, suburban and rural areas. As a result of the small number of respondents within each demographic type (age, qualification, clinic type), analysis at this level was not conducted.
Discussion
This study was undertaken to assist in answering a fundamental question about the body condition scoring of veterinary nurses currently working in different geographical areas (city, suburban and rural) in New Zealand to identify whether that would be a factor in any potential difference in body condition scores being assigned. It was hypothesised that city-based veterinary nurses would ‘normalise’ obesity in canine patients because of these patients anecdotally being over-represented in the dogs presented to veterinary practice.
The overall demography of participants matches what is observed in practice and is consistent with recent surveys of New Zealand veterinary nurses (Kongara et al, 2016; Harvey and Cameron, 2020). Over 70% of veterinary nurses worked in an urban area (suburban and city). This would match what is anecdotally known by the primary researcher about the veterinary industry in New Zealand, with a large number of veterinary clinics being in the large urban centres, however, there are no official data on the distribution of veterinary clinics versus population bases for New Zealand. Over half of respondents (44.1% suburban, 14.3% city; n=45) grew up in an urban area, with 41.6% (n=32) growing up in a rural area.
Two-thirds of respondents (66%; n=51) work in a companion animal practice with the remainder (34%; n=26) working in mixed practice. No respondents from equine-only or large animal-only practices responded. This likely reflects the fact that most equine and large animal clinics are mixed practices seeing farm/equine and companion animals.
Statistical analysis of the body condition scoring results with Kruskal-Wallis testing revealed no statistical difference between body condition scoring across the three current and childhood geographical areas. From a clinical perspective, this is reassuring as this indicates consistent scoring between veterinary nurses, regardless of the geographical area they currently work, or of childhood influences of growing up in a rural, suburban, or city geographical area. This is critical in terms of the consistent messages given to pet owners regarding their pet's health, with a particular focus on weight and nutrition.
As with any study, there were some limitations. The study only looked at the differences provided in body condition score. Another key component of the nutritional assessment is muscle scoring. Muscle condition scoring requires palpation of an animal, as opposed to a body condition score which can be accurate via visual assessment alone, with research showing there to be reliability in the nature of the assessment tool, even when body condition score assessment has been made using photographic images, rather than a visual inspection of a live animal along with palpation (Gant et al, 2016). As such, muscle condition scoring was not able to be included as part of this study. This would be an important topic for future research. A further limitation was that the WSAVA 9-point scale was not provided to participants as part of the survey, therefore veterinary nurses unfamiliar with this particular 9-point scale may have had difficulty accurately assigning a score to each image. In future iterations of this survey, the WSAVA Global Nutrition Toolkit scale will be included.
All survey respondents were female. Having all female respondents is representative of the industry, with most veterinary nurses in New Zealand being female (Harvey and Cameron, 2020). Research also shows a response bias toward female participants (Cull et al, 2005; Smith, 2008).
A sample size of 77 was achieved (once invalid responses were removed). This provides a 10.97% margin of error (Raosoft.com, 2020). A larger sample size would have provided more data, however the lack of any statistical difference within the group means the results obtained are still valuable when looking at the overall clinical relevance of the data. For a 5% margin of error, a sample size of 326 would be required.
Dissemination of the survey was via online social media platforms of the primary researcher, with participants encouraged to share within their networks. This yielded a poor response rate despite similar dissemination methods providing adequate sample sizes for surveys of New Zealand veterinary nurses in the past, with one main difference being that the current research project survey was not sent via email directly to NZVNA members (Harvey and Cameron, 2019). For future studies that focus on New Zealand veterinary nurses, this email to members may be critical to gaining a sufficient number of responses. It is also possible that New Zealand veterinary nurses did not see value in the project to warrant them spending time completing it. Whether this was inherent in the subject matter or because of insufficient marketing of the survey is unknown.
Consistent body condition scoring of veterinary patients in clinical practice is key to having consistent messages portrayed to owners. With a nutritional assessment becoming one of the five vital assessments and the WSA-VA Global Nutrition Toolkit abeing released in 2011, it is clear that from a veterinary health perspective, nutritional assessment and subsequent communication of findings and recommendations are important. Consistency in body condition scoring across veterinary nurses in the same veterinary practice, in different veterinary practices, and across different geographical areas is important to ensuring that consistent message. The research sought to provide clarity and reassurance around the consistency of body condition scores assigned to canine patients in a veterinary clinic setting by veterinary nurses, to aid in the accuracy of nutritional advice provided to clients regarding their pets. The results show that there is consistency in scoring. It is hoped that this information is being correctly and consistently provided to pet owners by veterinary nurses in New Zealand to support pet owners in managing their pet's weight.
Conclusions
With the obesity epidemic in companion animals being a cause of poor health and welfare, addressing this requires multiple approaches. One of those is ensuring the information provided to owners about the health and nutritional status of their pets is accurate and consistent. This study indicated consistency in the body condition scoring by veterinary nurses across a range of current and childhood geographical area settings (city, suburban, and rural). The lack of any statistical difference in the body condition score provided between these veterinary nurses provides clinical strength in the process of body condition scoring using a 1–9 scale.
While consistency in body condition scoring between veterinary nurses in different geographical areas is important, it is also key to ensure different members of the veterinary healthcare team are scoring patients the same. A future study looking at any differences between veterinarians and veterinary nurses would be the next step, possibly extending that to receptionists if they are undertaking this task in practice (as anecdotally, most veterinary receptionists in New Zealand have some form of animal care/veterinary nursing training).
This was a novel study that adds to the small body of knowledge that currently exists on this topic and helps to pave the way for future studies to continue to grow our knowledge around the impact of the veterinary industry on canine obesity and improving the health and welfare of companion pets.