
Canine ear disease is a common presenting sign to the veterinary surgeon in primary care practice. While the management of otitis is not difficult; managing it well to produce a complete resolution of the disease and prevent recurrence can be more challenging. The veterinary nurse can play an important part in helping to manage ear disease. In order to treat ear disease effectively it is essential to have an appreciation of the fact that for every ear problem there is a primary cause, almost always a secondary infection, and both predisposing and perpetuating factors are present. The most important primary cause of otitis is allergy (Paterson, 2002; Saridomichelakis et al, 2007; Zur et al, 2011). Allergic triggers include atopic dermatitis (CAD); cutaneous adverse food reactions (CAFR) and contact allergy/irritancy. Of these CAD seems to be the most common being the primary cause of otitis in up to 75% of cases in one study (Paterson, 2002). Precise figures for other allergic triggers of otitis are not available in the literature but are, in the author's experience, far less common causes of disease.
Clinical presentation of allergic otitis
Most dogs with CAD as their primary cause for ear disease develop otitis between 1 and 5 years of age with 31% presenting with ear disease before 12 months of age (Zur et al, 2011). Breed incidence for otitis due to CAD or CAFR tend to mirror the same breeds that are predisposed to allergic skin disease. The breeds with the highest risk of developing atopic otitis vary between areas and countries, with the local gene pool. At the author's clinic in the North of England, atopic otitis is seen most commonly in the Labrador, German Shepherd dog, Cocker Spaniel, Boxer, Golden Retriever and West Highland White Terrier. There are much fewer references to breed incidence of dogs with CAFR than CAD. According to some sources the Labrador is over represented in this allergic group (Rosser, 1993). Many dogs with allergic otitis will have a history of previous episodes of otitis possibly even with some form of seasonal incidence. They often also have involvement of other areas of skin, e.g. pedal saliva staining, periocular erythema and alopecia or recurrent ventral pyoderma (Favrot et al, 2010). On rare occasions only the ear is involved. Otic signs in both CAD and CAFR start on the ear pinna with erythema (Figure 1) and associated pruritus. They usually present with rubbing or scratching of their ear pinna often with head shaking. In many cases there is minimal involvement of the external ear canal at this stage and cytology of the ear pinna and examination of ear wax is normal. As allergic otitis progresses erythema is seen within the vertical canal extending down the ear to involve the horizontal canal and then the tympanic membrane. Many dogs with ear disease associated with hypersensitivity will have marked oedema of the pars flaccida (Figure 2) (Paterson, 2013), the vascular strip of the tympanic membrane. As the allergy becomes more chronic, proliferative changes develop in the ear and an inflammatory infiltrate forms. Initially this is mild and cytology reveals large numbers of keratinocytes with occasional inflammatory cells and no micro-organisms. As barrier function is compromised, infection occurs with either yeast or bacteria or both. Infection and ongoing inflammation lead to further changes within the canal which will become progressively more hyperplastic and narrowed (Harvey and Paterson, 2014a). Where topical drugs lead to signs of contact allergy or irritancy there is only involvement of the ears. In these cases dogs fail to respond to what is deemed appropriate topical therapy. Initially the area around the external auditory meatus becomes erythematous and pruritic, but if the topical drug is not stopped it will progress to become painful and ulcerated and can go on to develop severe bacterial infection (Harvey and Paterson, 2014a).


Investigation of allergic otitis
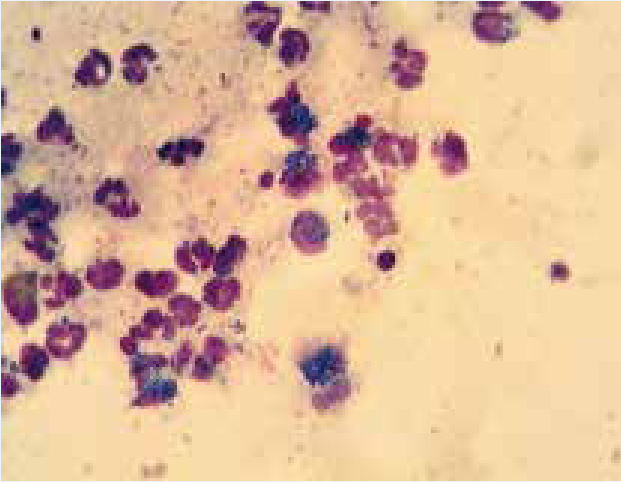
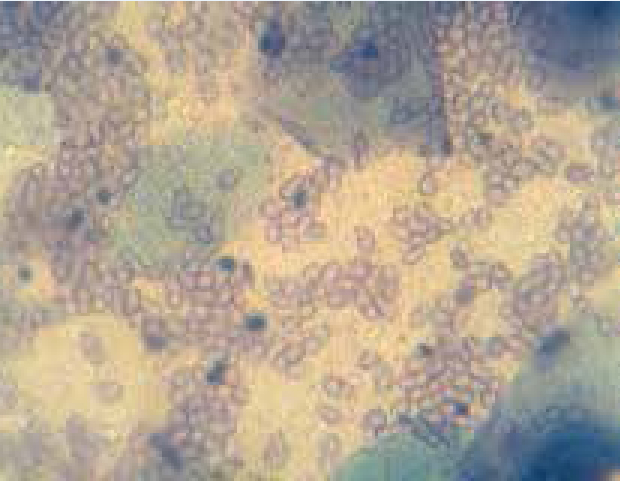
Ectoparasites are an important differential diagnosis for allergic otitis, especially in young dogs. Both Otodectes cynotis and Demodex spp. can be found in the ears of dogs (Neves et al, 2010; Harvey and Paterson, 2014a). Ear wax can be collected from the external ear canal on a cotton tipped swab, rolled along a microscope slide and examined, initially unstained, microscopically under low power. O. cynotis is an oval shaped mite with short pedicles and suckers on the distal end of each leg. Adult females are 350–450 μm in length, adult males are slightly smaller and can be seen actively moving through the wax. Eggs are large and oval (about 200 μm in length) and can also be seen within the ear wax. Demodex canis, a long, thin, cigar shaped mite 180–210 μm in length, is the demodex mite most commonly found in ear wax. It is very immotile on samples. Its eggs are fusiform (lemon) shaped. Samples of wax may also be rolled onto a slide and stained with Diff Quik to look for infection. In acute cases cocci usually Staphylococcus spp. (Figure 3) or Streptococcus spp. can be identified with or without yeast. In more chronic cases rods (e.g. Pseudomonas spp., Corynebacterium spp., and Escherichia coli) can be found either in isolation or with cocci or yeast. Yeast infection in ears is most commonly seen with Malassezia pachydermatis a large peanut shaped organism (Figure 4).
Where contact allergy problems can be ruled out on the basis of a history and clinical examination CAFR and CAD need to be investigated. A carefully taken dietary history can help formulate an appropriate hypoallergenic diet. The author favours a hydrolysed complete veterinary diet of which there are many excellent ones on the market which should be fed for a minimum of 4 weeks. Although hydrolysed diets are an excellent diagnostic tool they can be slightly unpalatable for some dogs who will not eat them. When this occurs a home cooked diet of a novel protein or carbohydrate source may be substituted. A diagnosis of CAD is made by exclusion, on the basis of a compatible history, clinical examination and elimination of other potential primary causes. In vitro or in vivo allergy testing can be useful to identify specific allergic triggers which can benefit ongoing management of the disease.
Treatment of allergic otitis
Ear cleaning forms an important part of the therapy of allergic otitis. It helps make the dog more comfortable, removes wax to aid better penetration of subsequent topical therapy, and allows visualisation of the tympanic membrane so that appropriate treatment choices can be made. It is important to assess the canal before selecting an ear cleaner. Many dogs with allergic otitis have sensitive ear canals (Figure 5) and will react adversely to cleaners that contain potent ceruminolytics (sodium docussate, squalene, carbamide peroxide), alcohol, astringents or acids. Where there is any doubt as to whether a dog will tolerate a particular cleaner, it is often prudent to use a small amount of a cleaning solution in the dog's ear in the consulting room to see how it reacts to the product, before dispensing a whole bottle. Where ears are waxy and sensitive then gentle ceruminolytic products should be selected including those with a propylene glycol or oil base. Topical prescription ear drops can often be prescribed empirically after cytology has been performed (Harvey and Paterson, 2014b). Where yeast is identified suitable treatment may contain nystatin, miconazole, clotrimazole or posaconazole (Harvey and Paterson, 2014b). When cocci are found on cytology therapy might include aminoglycosides (gentamicin, framycetin), fusidic acid or flurfenicol (Harvey and Paterson, 2014b, Paterson, 2016). Where rods are detected, especially if a Diff Quik rather than a Gram stain is performed, then a sensitivity profile is less predictable and culture is important to help decide on appropriate therapy. If CAD only affects the ears and the dog is compliant then ongoing therapy after the resolution of the infection may be achieved with topical glucocorticoids. Glucocorticoids are hugely beneficial in allergic otitis (Paterson, 2016). Their anti-inflammatory effects help reduce neutrophil chemotaxis and hence the formation of an inflammatory infiltrate. They reduce inflammation within the ear canal to reverse the hyperplastic change induced by the allergic reaction. They also reduce ceruminous gland production to dry up wax within the ear. Due to the fact that many topical otic drugs combine an antibiotic with a glucocorticoid, some dermatologists prefer to use an off license topical glucocorticoid preparation to provide anti-inflammatory effects without chronic antibiotic usage. Topical glucocorticoid eye drops or cutaneous glucocorticoid sprays may be used for ongoing therapy (Paterson, 2016); these appear to be quite safe providing the ear drum is intact. As an alternative, injectable glucocorticoids can be added to antiseptic ear cleaners to provide a combined antipathogenic/antiinflammatory therapy (Paterson, 2016).

Where the dog is not amenable to topical therapy or the owner is unable to apply these types of drugs, then systemic therapy may be needed. Oral drugs such as ciclosporine, janus kinase inhibitors and glucocorticoids can be prescribed to control CAD. Although both ciclosporine and janus kinase inhibitors are useful to control allergic pruritus, neither have the same anti-inflammatory effects in the ear as glucocorticoids and so are often best suited to controlling more generalised CAD and not allergic otitis. Despite this though there are dogs that do derive benefit from these types of drugs. Often low dose alternate day prednisolone is better maintenance therapy in dogs that will not accept topical medication (Morris, 2004). When used to treat CAD the author will generally start any of the systemic drugs at a full therapeutic dose rate but reduce medication to the lowest possible maintenance dose rates, to prevent recurrence of the disease, once initial control has been produced.
Allergen specific immunotherapy (ASIT) based on either in vitro or in vivo allergy test results can be used successfully to control otitis in cases of CAD. This can be administered as either a subcutaneous injections (subcutaneous immunotherapy, SCIT) or sublingual drops (sublingual immunotherapy, SLIT) and can be used as the sole form of therapy to control recurrence of pruritus and infection in dogs with ear disease. Although it will work without any other forms of treatment the author will where possible supplement either SCIT or SLIT with ear cleaning solutions.
In all cases of allergic otitis it is important that owners are made aware that the dog will need long-term therapy. This may be maintenance of a low allergy diet with regular use of a cleaning solution; ASIT with a topical cleaning solution and topical glucocorticoids or anything in between. Allergic otitis like CAD can have a seasonal pattern and good client care should include regular rechecks to ensure the dog remains comfortable. Rechecks are best scheduled for times of the year when animals have had problems in the past. Otoscopic examination of the canal and cytology both give useful indicators as to the stability of the animal's ear condition. Nurse clinics are a useful place for this to be performed and allow deterioration in the dog's ear condition to be picked up at an early stage so that veterinary intervention can be more effective.
Conclusions
Allergic otitis is the most common primary cause of ear disease in the dog. The veterinary nurse can play a valuable role in helping to investigate allergic otitis. Cytology of aural discharge performed by nurses to identify parasites such as Demodex spp. and O. cynotis can help in the selection of topical therapy. Where cytology identifies aural infection, the nurse's findings can contribute to selection of appropriate topical therapy. When CAFR are suspected as a primary cause of otitis, then the nurse can discuss options with clients for a home cooked hypoallergenic diet or discuss the benefits of a hydrolysed diet and the need to strictly adhere to the prescribed dietary regimen. Specific allergy testing can be helpful to identify environmental trigger and allow formulation of vaccines if needed. Client instruction on the most appropriate ear cleaners for their pet's condition and the best way to clean ears successfully can be undertaken by the practice nurse. Ongoing management in allergic otitis should include regular recheck to ensure there is no relapse of the condition and ensure clients have appropriate therapy for ongoing treatment. This can be performed through nurse clinics and clients can be redirected back for veterinary assessment where routine check-ups identify changes in the status of the pet's ear.