Bite wounds are some of the most common traumatic injuries encountered in veterinary practice, with bite wounds in cats and dogs accounting for 10% to 15% of all veterinary traumas in emergency clinics (Kolata et al, 1974; McKierman and Adams, 1984; Seibold, 2004). The degree of severity of bite wounds varies depending on the animals involved, the body condition of the animal, any concurrent medical conditions, e.g. immunocompromised patients, the locations of the wounds, the depth of the wounds, and the amount of underlying tissue damage. The ‘big dog versus little dog’ or ‘dog versus cat’ are common presentations to veterinary practices. The time lapse between injury and presentation, will often dictate the medical and surgical management of the case.
Animals that have suffered multiple bite wounds with deep tissue damage may suffer severe systemic effects. If the animal survives the initial attack, they often present to the hospital in profound shock and require aggressive volume resuscitation, e.g. shock rate fluid boluses of 60–90 ml/kg, before wound management can be thoroughly addressed, in order to correct underlying hypovolaemia and restore perfusion.
The initial treatment of these patients depends on the severity of the injuries; the patient's major body systems should be assessed, with particular attention to cardiovascular, respiratory and neurological examinations, and the patient's condition evaluated before commencing wound treatment or repair. Depending on the nature of the underlying injuries, staff should provide oxygen supplementation, and be prepared to carry out intubation and ventilation, or even assist with tracheostomy, thoracocentesis or thoracostomy tube placement as required. Major body system clinical parameters should be monitored closely; noting a change in the trend of these values can alert the clinical team to the need to adjust a treatment plan early and effectively before the development of devastating conditions such as systemic inflammatory response syndrome (SIRS), acute respiratory distress syndrome (ARDS), disseminated intravascular coagulation (DIC), multiple organ dysfunction syndrome (MODS).
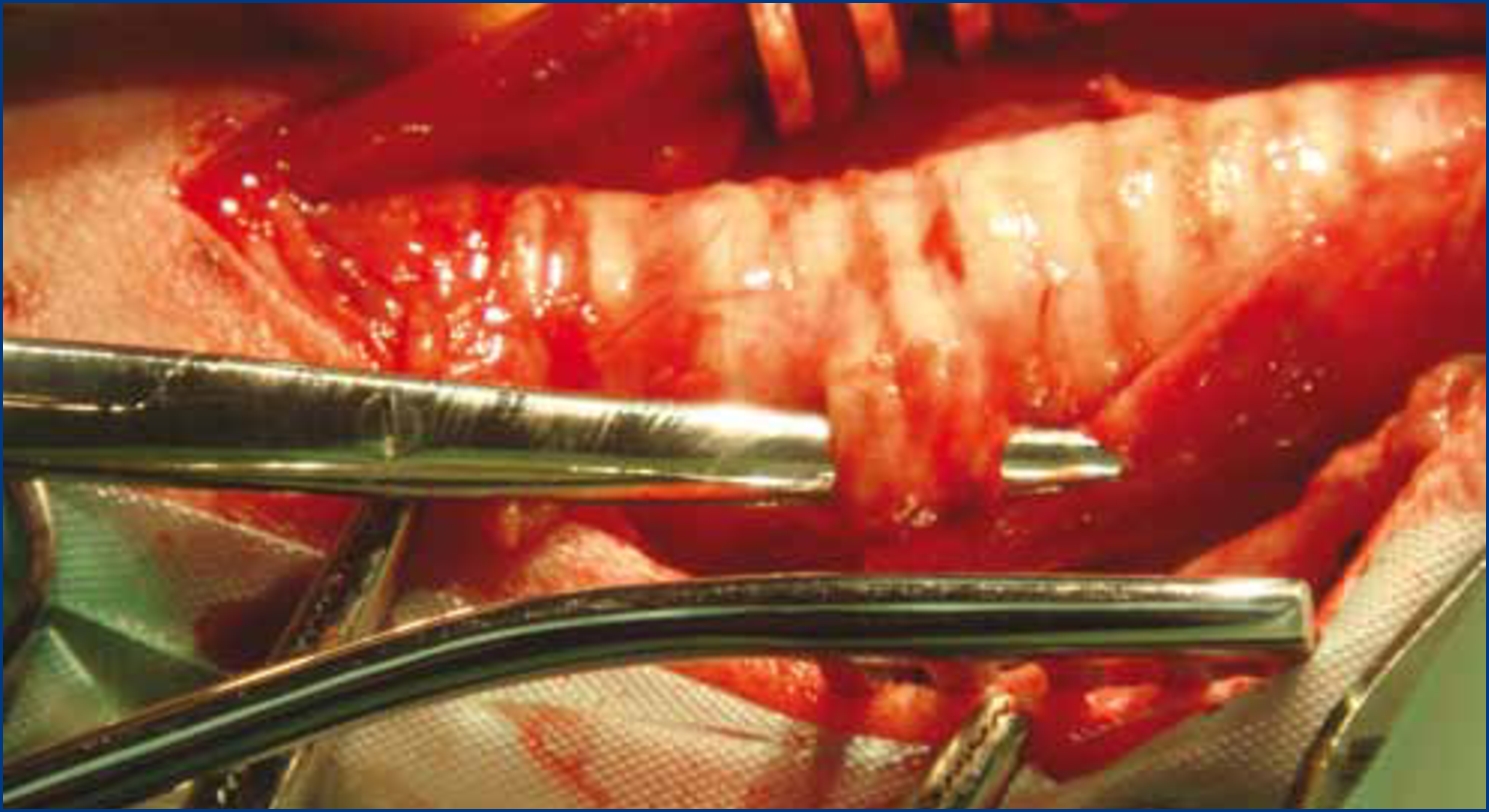
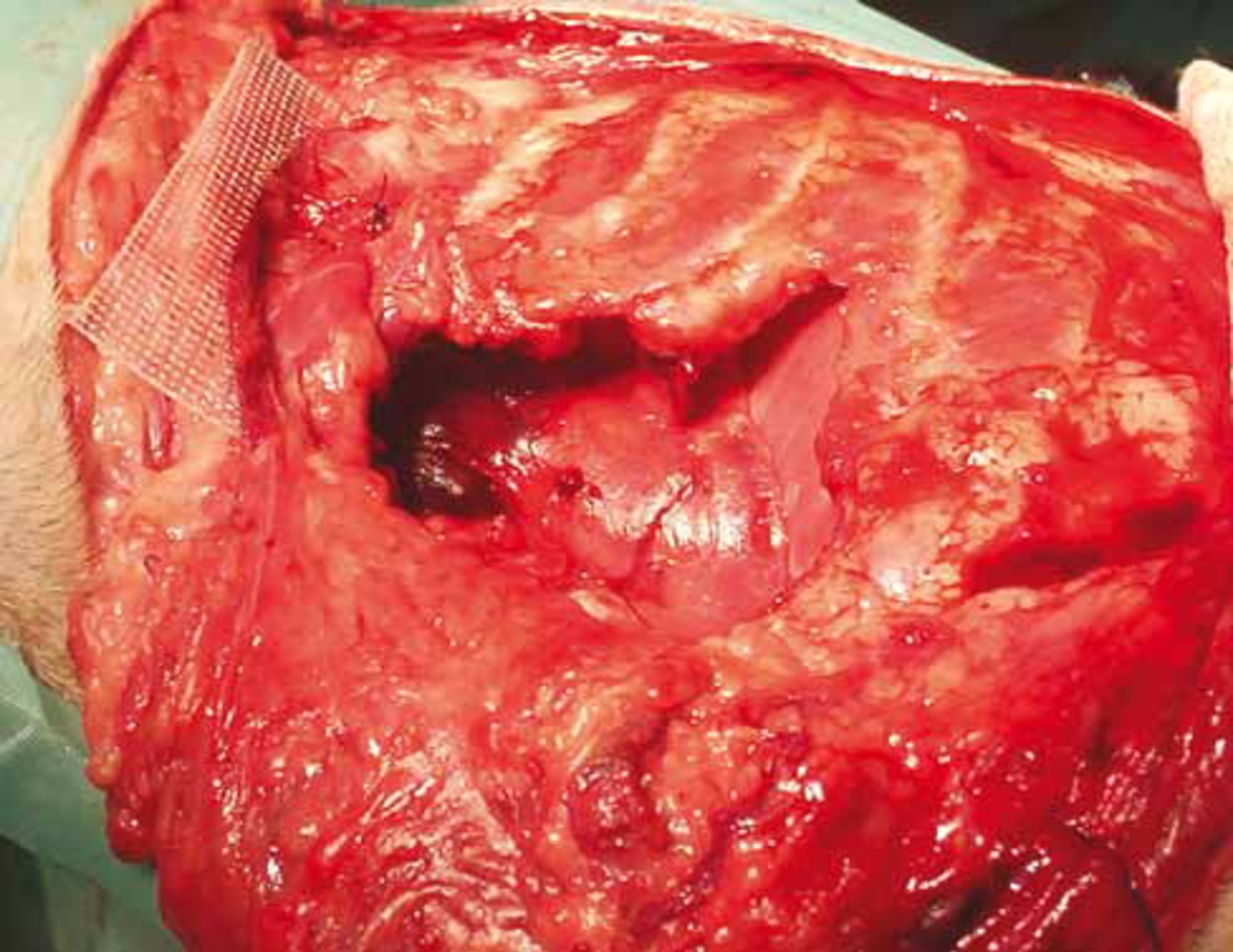
Only very rarely do bite wounds result in the laceration of a major blood vessel which requires immediate anaesthesia and repair, although they will require initial debridement, lavage and dressing placement. In contrast, bite wounds resulting in trauma to the trachea (Figure 1) or chest wall (Figure 2), can result in respiratory compromise of the patient, and a life-threatening situation which requires immediate intervention. It is common for the attacking animal to pick up the smaller animal and shake it back and forth. This results in tremendous trauma to the underlying tissue and muscle, although the puncture wounds through the skin itself may look a lot less significant. Thorough evaluation of any animal with such bite wounds to the chest with or without respiratory compromise is essential. On initial examination following an initial flush and clean, small wounds should be covered with a sterile dressing and bandaged appropriately, and larger wounds kept moist, e.g. using a hydro-gel, and also covered with a sterile dressing, until more extensive cleaning and debridement can be performed.

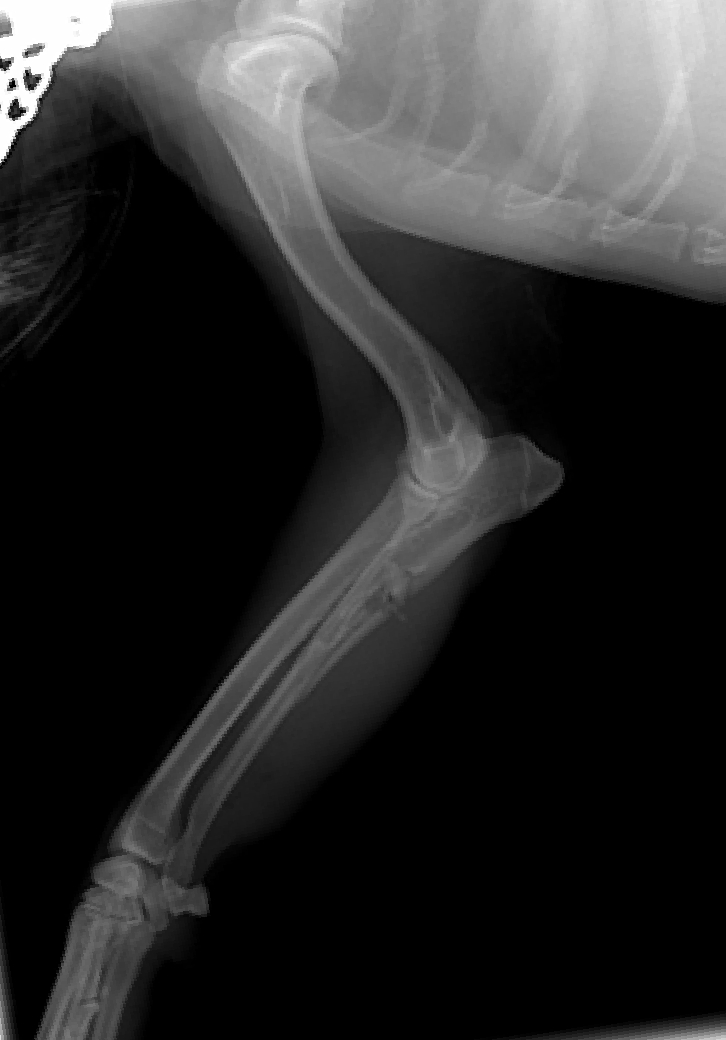
If a wound penetrates the thoracic cavity (Figure 3), this is likely to result in a pneumothorax, lung contusions or lacerations, haemothorax or thoracic tracheal trauma (Davidson, 1998). Again thoracic wounds should be dressed appropriately, depending on the severity of the wound, and the pneumothorax/haemothorax drained via needle thoracocentesis, repeatedly if required; in severe cases, the placement of a chest drain may be required. If at all suspicious radiographs of the patient's thorax and abdomen should be obtained.
Bite wounds to the head require cranial nerve and central nervous system (CNS) evaluation, which may be assessed during the initial major body systems assessment of the neurological system. Neck bite wounds raise concerns about laryngeal, pharyngeal, cervical trachea, and oesophageal injury. Endoscopy of the oesophagus and trachea is indicated when there are deep wounds of the neck and action taken as required, in order to rule out underlying damage to these structures.
Analgesia
A multi-modal approach to analgesia should be selected in the bite wound patient, the first line analgesic of choice being an opioid, either pure agonist, such as methadone or morphine, or a partial agonist such as buprenorphine. In severe cases where such analgesics do not appear to be providing a sufficient level of analgesia, then a constant rate infusion (CRI) combining different analgesic drugs may be selected. In additional to systemic analgesics, local anaesthetics in the form of regional blocks for example to the rib area or to a severely traumatized limb can dramatically reduce the need for more analgesics.
Non-steroidal anti-inflammatory agents (NSAIDs) will help with post-operative pain but it should be ensured that the patient be adequately hydrated and normotensive before NSAIDS are administered in order to prevent detrimental effects to the renal and gastrointestinal systems.
Inflammation and trauma
Whenever dealing with severe bite wound patients it should be remembered that patients with severe tissue trauma are at risk of excessive activation, or loss of control of, inflammation. This can lead to the development of SIRS, which may progress to DIC or ARDS (Holt and Griffin, 2000).
The issue of infection also needs to be considered. All bite wounds should be considered contaminated (Harari, 1993) whether they are open (skin penetration) or closed (skin crushed) and contain a polymicrobial flora that reflects the aerobic and anaerobic bacteria in the oral cavity of the biter, skin of the victim, and environment (Brook, 2005). In cats and dogs, Pasteurella multocida is the most common pathogen cultured (Goldstein and Richwald, 1987; Talan et al, 1999). Although cat bites are more likely to become contaminated than dog bites (Goldstein and Richwald, 1987; Lewis and Stiles, 1995) by virtue of the sharp-pointed teeth of cats producing puncture wounds that can inoculate bacteria into underlying tissue, dog bites tend to be more problematic for the veterinarian because of the combination of crush, tear, and avulsion injury. All bite wounds place the patient at risk of sepsis.
If the wounds are severe enough, and perfusion deficits are present, then SIRS/sepsis can result in MODS. Sepsis can be defined as the systemic inflammatory response to infection with bacteria, or viral, fungal or protozoal organisms; SIRS is the clinical manifestation of the patient's response to severe injury, microbial invasion, severe inflammation, or neoplasia (Powell, 2011). Bite wound patients are more susceptible to these conditions because of the nature of the injuries sustained. MODS describes the presence of organ failure, coagulation abnormalities, and cardiovascular derangements that occur due to the presence of sepsis and SIRS (Powell, 2011).
Local tissue damage
The canine jaw can exert a force of 150 to 450 psi (Pavletic, 2002; Goldstein and Richwald, 1987; Swaim and Henderson, 1992). The incisor and canine teeth can apply shearing forces to the skin when applied perpendicular to the skin surface, sharply dividing the tissue as they are drawn through it. At angles less than 90°, the tensile forces can create avulsion of the skin, together with hernias and devitalization of the underlying tissues. Compression forces generate the ‘classic’ puncture wounds seen with canine teeth, or crushing wounds of premolars or molars.
Wound care
Following adequate analgesia and/or local anaesthesia sterile water soluble lube should be placed into the wound. This helps prevent additional contamination of the wound and aids in the removal of hair and debris following clipping the area. It is very important to clip a wide area around the puncture wound, if the margins of the pocket can be delineated then clipping an additional 5–10 cm beyond the margin of the wound is recommended. The shaved area is then scrubbed with an antiseptic scrub, e.g. using a 0.5% chlorhexidine gluconate solution when likely to come into contact with broken skin. Wound edges that are discoloured, cold, and lack blood supply are identified for removal once anaesthesia has been induced. It is not necessary to undertake most bite wound explorations in an aseptic operating room environment. That said if the animal requires chest or abdominal exploration then standard aseptic techniques should be carried out in an operating room environment. Each wound should be cleaned and flushed with copious amounts of an isotonic sterile solution. Lactated Ringers is considered to be a more suitable flushing solution than 0.9% NaCl because the pH is closer to that of normal tissue. 0.9% sodium chloride has a pH of 5.4 whereas lactated Ringers solution has a pH of 6.3 (DiBartola and Bateman, 2006).
Once the patient is considered haemodynamically stable, then anaesthesia should be performed in order to carry out exploration, lavage and debridement of the wound. The extent of damage as a result of bite wounds is often underestimated, therefore the anaesthetist should be prepared for prolonged anaesthetic times, and therefore should prepare accordingly. These patients may become haemodynamically unstable during anaesthesia, so close attention should be paid to perfusion throughout surgery, e.g. monitoring of arterial blood pressure, blood gas analysis and/or measurement of urine output.
Small puncture wounds that have less than a centimetre of pocketing can be flushed and left open to heal by second intention (Seibold, 2004). Wounds that have more than a centimetre of pocketing or evidence that the bite wound has disrupted the underlying subcutaneous tissue and/or muscle layers must be opened and explored. Deep puncture wounds are best explored by opening the subcutaneous pockets the length of the wound and visualizing the underlying tissue. Just placing a drain the length of the wound can be inefficient if there is underlying muscle damage and devitalized tissue remaining (Seibold, 2004). Often the wound that is below the skin is much more severe than can be appreciated from a small puncture through the skin. If there is not an actual puncture wound to the skin but there is marked bruising and/or pain in the area it is recommended to explore the region (Seibold, 2004) by opening the skin and identifying the margins of the wound, in combination with debridement and lavage (Figures 4 and 5).

Any wounds into the neck, chest wall, abdomen, or groin area should be opened and evaluated for penetration of the chest or abdominal cavities. When exploring wounds over the thorax the anaesthetist should be prepared to instigate intermittent positive pressure ventilation (IPPV) immediately in the event of an open pneumothorax being discovered. Commonly bite wounds have entered the thoracic cavity without evidence of a pneumothorax on radiographs, torn muscle or fat ‘plugs’ the hole, and when this is disturbed during exploration, air is drawn through the wound into the chest (personal experience). All bite wounds that result in a puncture to the abdominal cavity must be followed with an exploratory laparotomy to assess the damage to the abdominal organs and gastrointestinal system. The crushing forces that the animal may have suffered can result in intestinal compromise that may result in devitalization of the tissue in 12 to 72 hours, resulting in septic peritonitis in the patient (Seibold, 2004). In patients with multiple traumatic wounds serum total protein (TP) should be closely monitored during the following days, as these patients can easily become hypoproteinaemic, additionally the lavaging of body cavities, i.e. abdomen, will further add to loss of serum total protein.
Post-operative considerations
Post-operative management of these patients includes management of pain, antibiotics, repeated monitoring of specific diagnostics, nutritional support and good nursing care.
Post-operative monitoring ideally should include continuous electrocardiogram (ECG) and arterial blood pressure, hourly temperature, pulse, respiration (TPRs) should be monitored, and ideally urine output measured. Pulse quality, limb temperature, respiratory pattern, capillary refill time and mucous membrane colour should also be assessed at the same time along with monitoring of packed cell volume (PCV)/TP, glucose, electrolytes, lactate, complete blood count (CBC) and platelet counts. Serum albumin levels should also be measured should TP drop. Careful monitoring of these parameters is vital in terms of alerting staff to changes in the patient's condition and allowing changes to be made to the patient's treatment plan.
Nutritional support should also be considered and addressed as soon as possible. The provision of early nutritional support for these patients is essential for healing and recovery. Early placement of oesophogostomy or gastrostomy tubes should be considered if anorexia is likely to occur. Special consideration should also be given to the overweight feline patient. Feeding is very important as feline patients are at risk for the development of hepatic lipidosis. Cats with multiple wounds, especially those that involve the fat pads of the ventral abdominal area require very close attention and monitoring. These patients will often appear much brighter following resuscitation and wound repair only to succumb to SIRS or sepsis 48 to 72 hours after presentation (Seibold, 2004). The development of icterus, bradycardia and/or persistent hypothermia is a grave sign and immediate changes in the treatment plan should be instituted.
Conclusion
Bite wounds are commonly seen in small animal practice and these patients should be treated holistically, paying close attention to their major body systems and degree of hypovolaemic shock on initial presentation. Close monitoring of the patient's vital signs during the initial treatment will determine whether it is effective or not, and whether changes to the treatment plan. e.g. fluid therapy rates or analgesia, are required.