
For some time now it has been known that the mortality rates associated with anaesthesia in small animal patients are much higher than in human medicine (Brodbelt et al, 2008; Mellin-Olsen et al, 2010; Bainbridge et al, 2012). There has been a vast improvement over the last 20–30 years which has largely been prompted by advancements in monitoring methods and equipment, pharmacological advances and better understanding of the subject allowing better education and professional development (McMillan, 2014). Indeed the risk of anaesthetic-related mortality in a healthy (American Society of Anesthesiologists Physical Status Classification I-II) dog reduced from 0.11% to 0.05% between 1980 and 2003 (Clarke and Hall, 1990; Brodbelt et al, 2008). Despite this reduction the level of anaesthetic fatalities demonstrated by The Confidential Enquiry into Small Animal Fatalities (CEPSAF) fall far below those observed for human anaesthesia in both developed and developing world countries which were 0.000018% and 0.00012% respectively for the period 1990s to 2000s (Mellin-Olsen et al, 2010; Bainbridge et al, 2012). CEPSAF shows an overall risk of anaesthetic death (within 48 hours of the procedure) in small animal patients as: dogs 0.17%, cats, 0.24% and rabbits, 1.39% with post-operative deaths accounting for 47% of the deaths in dogs, 61% in cats and 64% in rabbits (Brodbelt et al, 2008).
The pursuit of patient safety
There is no doubt that the pursuit of patient safety must address the current gap between best practice and the care currently given to veterinary patients (Weller and Merry, 2013). However, when most practices discuss their anaesthesia protocols it is very much with a view that ‘nothing died’ so there is the assumption that their anaesthetic processes and choices are ‘fine’. There is also, often, an assumption that anaesthetic fatalities are somewhat inevitable, yet this is a view that was challenged in 1949 in human anaesthesia by Robert Macintosh who contested that they were frequently attributable to anaesthetists’ failure (Weller and Merry, 2013). So is it good enough to still hold these outdated viewpoints of veterinary anaesthesia? Or should veterinary professionals be pushing the quality curve forwards, striving to achieve an evidence-based best practice approach to anaesthetic safety for all the patients under their care? What should they be doing about the critical incidents and adverse events, including the near misses and human errors, which happen every day in veterinary practice? In the majority of cases these do not result in death but they undoubtedly increase risk so shouldn't veterinary practices be working to put systems and training in place to minimise them?
The last 10–15 years have seen patient safety become one of the cornerstones of human medicine in particular with regard to human anaesthesia and critical care. The publication of the Institute of Medicine report ‘To err is human’ (Kohn et al, 2000) publicised the fact that between 40 and 100 000 patients were dying, not from their disease processes, but from medical errors made by the doctors and nurses treating them. The report drew on research from the aviation and nuclear power industries and for the first time human factors, and the failure of cognitive processes in diligent professionals that result in error, were recognised. This was closely followed by the publication of ‘An organisation with a memory’ (Department of Health, 2000) and the focus on patient safety in healthcare and then specifically anaesthesia began in the UK. Much of this has revolved around clinical auditing, something that (despite being a mandatory part of the Royal College Veterinary Surgeons (RCVS) practice standards scheme) is still truly sparse in veterinary medicine. Patient safety in veterinary medicine is very much in its infancy with no official reporting systems or clinical governance yet in place despite a number of recommendations and mandates relating to the smaller aspects of the process. Oxtoby (2014) proposed that ‘veterinary practices, unlike the NHS hospitals, are often smaller, less fluid and less complex and have a greater advantage in the development and implementation of practices and policies tailored to ‘fit’ and ‘owned’ by those who work there to improve anaesthetic patient safety’. Emphasis is needed on the analysis of what went wrong and why instead of ‘who’ made an error. This allows a ‘just culture’ and encourages practitioners to feel safe to report their errors knowing that the aim is to improve safety rather than to blame the individuals (Weller and Merry, 2013). It must be recognised within the veterinary and veterinary nursing professions just how many preventable accidents and errors occur every day.
Preventable accidents and human errors
Consider the human errors that may have been seen numerous times in practice; wrong drug administered, wrong dose of the right drug administered, right drug and dose administered by the wrong route, wrong part of the patient clipped for surgery, mis-communication, incomplete clinical assessment, lack of knowledge of the drugs or equipment, equipment not set up correctly or failure not recognised, inadequate monitoring or failure to act on the readings obtained, misdiagnosis, airway mismanagement, fluid mismanagement, burns from the heat pads or diathermy, corneal abrasions or ulcers (McMillan, 2010). This list is not exhaustive but these are some of the adverse events that occur repeatedly due to human error. Before an action or inaction can be assigned as a ‘preventable error’ a judgment must inevitably be made that indeed the error was preventable, for example, if a catheter infection occurs following cephalic catheter placement was this preventable and the result of erroneous placement procedure? Or was it inevitable due to the patient's condition (Dekker, 2011)?
Reasons for human or preventable errors
Cognitive errors (including knowledge failure, mistakes and/or momentary slips in attentions) occur when the brain fails to identify and respond to a mismatch between intention and action (Hogan and Sanders, 2014). Knowledge failure can be remedied through education and experience but the ‘slips in attention’ where keys are mislayed, purses/wallets put in the fridge or the place where the car was parked forgotten are commonplace and occur in everyday life (Hogan and Sanders, 2014). Most anaesthetists would agree that these ‘slips of attention’ can occur throughout the day but often more so during the critical periods of induction and recovery from anaesthesia (Hogan and Sanders, 2014).
Human factors analysis recognises that many adverse events that occur are not a result of a lack of technical prowess or knowledge but through the breakdown of coordination between people and people and technology (Dekker, 2011). While it envelops the cognitive processes of the individual, as discussed, it does so in the context of the culture of the workplace, within the constraints of hierarchical boundaries and theorises that the major source of risk to patient safety lies not with the individuals but with the system surrounding and interacting with these medical professionals (Dekker, 2011).
The human factors approach allows analysis of the bigger picture of the veterinary professionals, the veterinary practice and practice culture, how ‘soft skills’ influence the safety culture and organisational risk. Anaesthetists non-technical skills (ANTs) refer to a particular set of skills, in addition to the acquisition of the appropriate knowledge and practical skills to ensure competent practice, such as communication, team work, planning, resource management, a drive to maintain knowledge, decision making, and a willingness to ask for help, that are used integrally with medical knowledge and clinical techniques (Armitage-Chan, 2014; Fletcher et al, 2002). Training in these skills has been widely recognised as an important contributor to safety, particularly in aviation but more recently in anaesthesia and surgery (Armitage-Chan, 2014).
Distraction has been identified as a major cause of accidents in aviation where pilots were distracted during critical phases of the flight process (Broom et al, 2011). The ‘sterile cockpit’ concept, which developed as a result of this, whereby pilots refrain from all non-essential conversation during the critical stages of flight at any time when the plane is at less than 10 000 feet, effectively take-off and landing, has since been applied to human anaesthesia (Broom et al, 2011). Induction of anaesthesia is often a calm, quiet and focussed time but in both human and veterinary anaesthesia recovery is often less so with noise levels from conversation, multiple conversation and music within theatre/recovery the possible cause of distraction or loss of concentration of the anaesthetist or nurse monitoring the patient (Broom et al, 2011). This time of reduced vigilance is something that should be of consideration to veterinary practitioners especially considering the high number of anaesthetic fatalities that occur within the first 3 hours of the post-operative period (Brodbelt et al, 2008).
Preventable errors occur every day in veterinary anaesthesia. The situations outlined in Box 1 will be sadly familiar to many of veterinary nurses and yet because none of them led to mortality of the patients concerned these accidents and errors are not reported, analysed and learned from.
Improving patient safety
The reason ‘WHY’ we need to improve patient safety in anaesthesia has been evidenced but the recognition of ‘HOW’ and by ‘WHO’ is often a stumbling block for practitioners wishing to make improvements. For this reason the Association of Veterinary Anaesthetists (AVA) has recently formed a patient standards subcommittee with a central aim to improve patient safety and welfare in veterinary anaesthesia. The first task of this subcommittee was to develop a veterinary anaesthesia checklist (Figures 1 and 2) and implementation manual for use in all veterinary practices. The checklist and implementation manual can be downloaded from: http://www.ava.eu.com/vets-and-nurses.
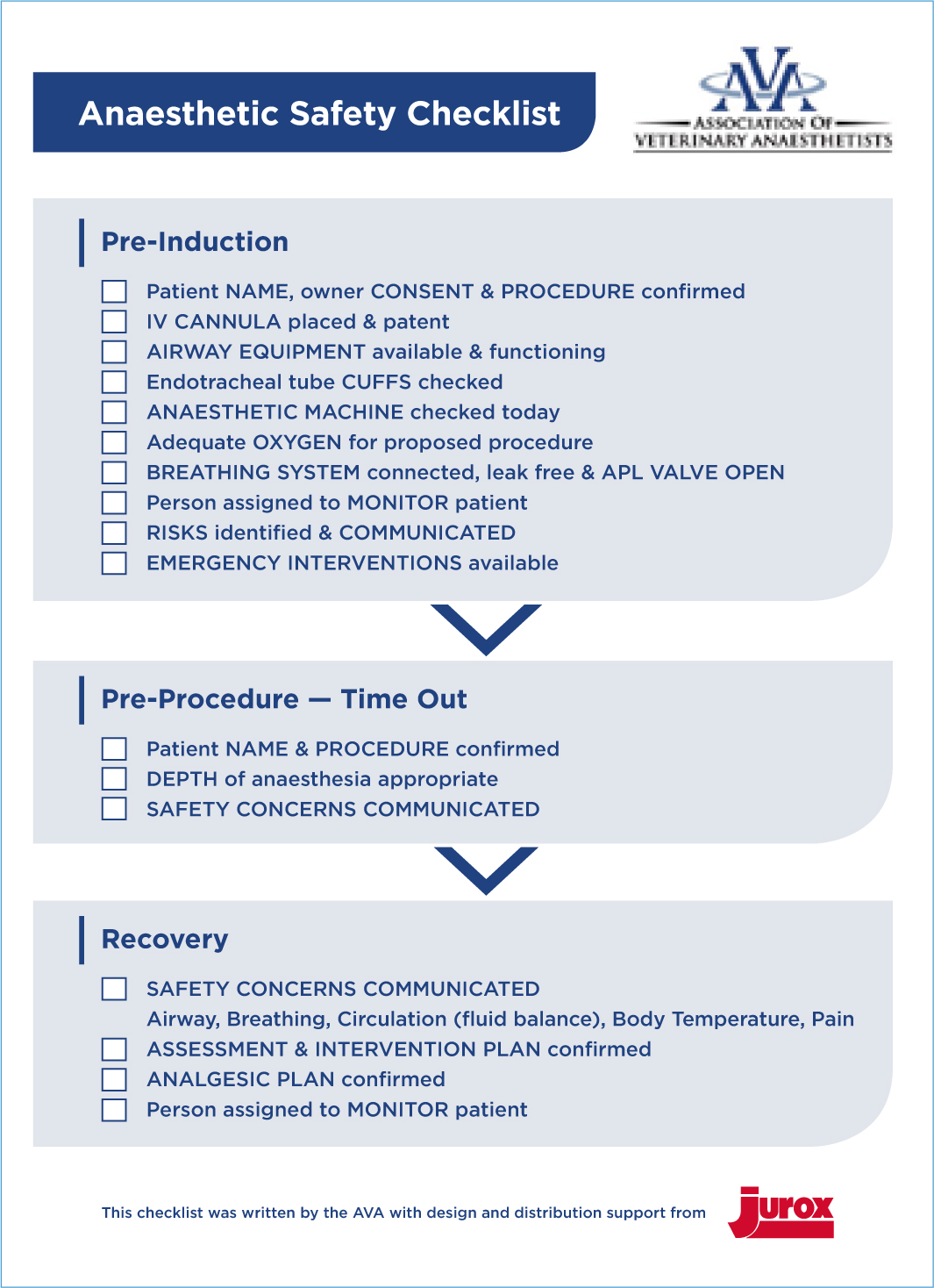
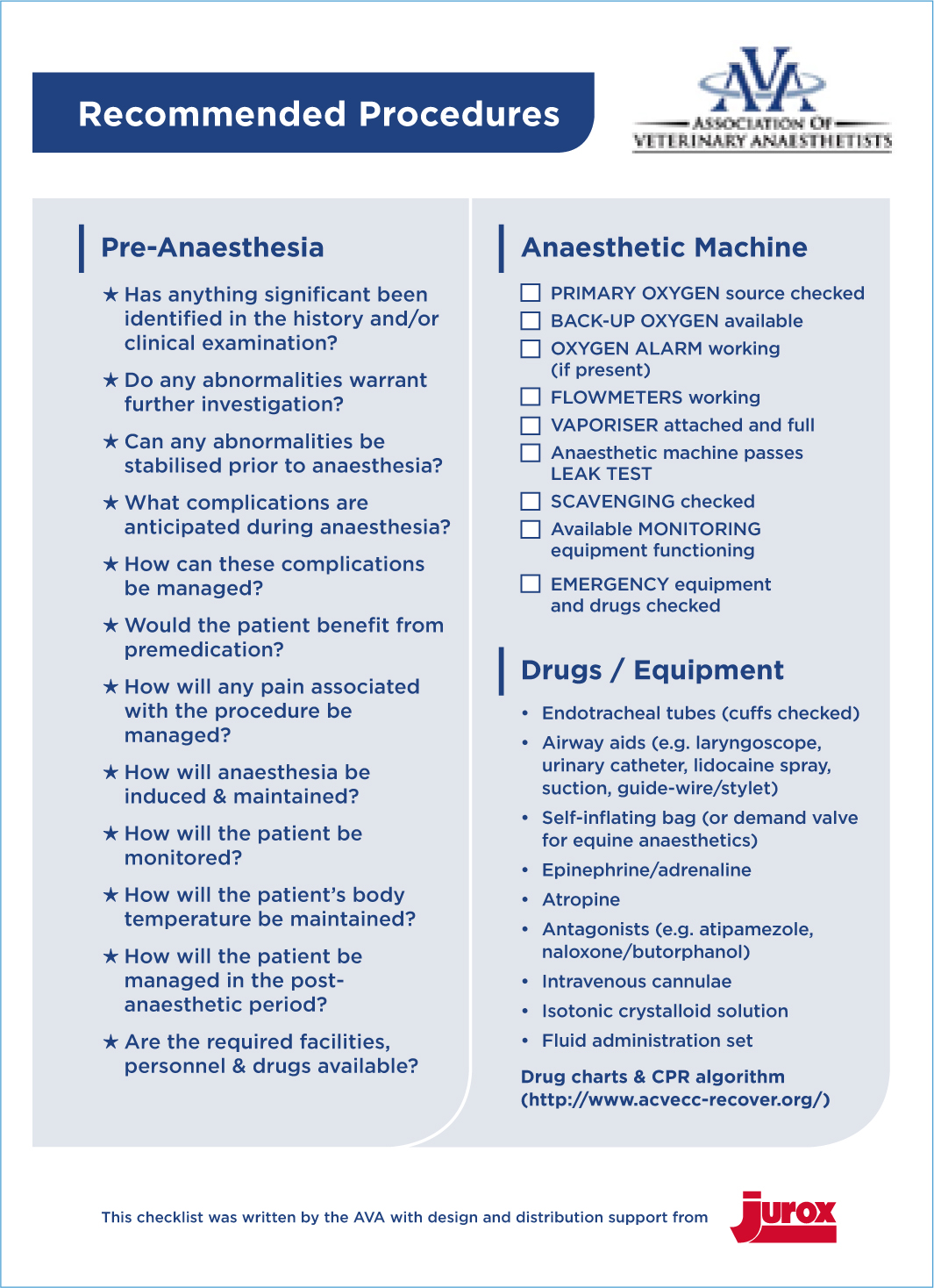
Checklists strengthen cognitive processes and have been shown to standardise, and make more predictable, the performance of teams despite a diverse range of individuals, situations and clinical environments (Gillespie et al, 2014). The use of a checklist such as that published by the AVA, provides a means of preventing accidents and incidents by providing a structure for improvement of non-technical skills, such as communication and team work, within the perioperative team and by ameliorating the influence of human factors (Armitage-Chan, 2014).
In addition to this, simulation training has been shown to improve performance in anaesthesia professionals compared to those having received didactic training (Chiu and Elliot, 2012). It is intuitive to veterinary nurses to perform preoperative anaesthesia machine checks yet machine faults are still missed regardless of anaesthesia experience (Chiu and Elliot, 2012) (Figure 3). Simulation training forms an essential part of the veterinary nursing observed clinical standardised examinations (OSCEs) and while this is also the norm in some of the veterinary schools in the UK this is not standard. This type of simulation training, where brief experiential training associated with a boost from repeated testing, is proven superior to the traditional lecture or didactic training (Chiu and Elliot, 2012). Therefore, surely it should be utilised as a foundation to anaesthesia education for both undergraduate veterinary surgeons and veterinary nurses? This model would allow standardisation across the UK and formation of a strong foundation that could be strengthened further by implementing a checklist mentality.


A nationwide reporting system for adverse events (including near misses) and critical incidents including mortality would be the ultimate aim for veterinary anaesthesia first within the UK and eventually globally. The primary purpose of the reporting of adverse events is to help veterinary professionals learn from experience (Leape, 2002). This is a process which should be familiar through the practice of reflection using the models of reflective practice taught within the current veterinary nursing syllabuses at both degree and diploma level (Welsh and Wager, 2013). This type of reporting system also has several other advantages including, but not limited to: prioritising hazards to allow appropriate resource allocation; earlier detection of unsuspected hazards due to identification of low-frequency events; and identification of common contributing factors (Leape, 2002).
Conclusion
In conclusion, a safe, patient-centred approach to veterinary medicine should be at the forefront of everything veterinary surgeons and veterinary nurses do with a particular emphasis on improving anaesthetic processes and protocols (McMillan, 2014). Evidence-based veterinary medicine by definition demands that the best available evidence is used in combination with clinical expertise to make the best decisions possible for clinical patients and clients (Bille et al, 2014). It has previously been demonstrated that application of evidence-based approaches and recommendations may significantly contribute to a decrease in anaesthetic mortality (Bille et al, 2014). There are now several instruments, a wide evidence base and a number of valuable resources, available to veterinary professionals to achieve this. This has been spearheaded by the publication of a veterinary specific anaesthesia checklist and guidance booklet by the AVA alongside a significant increase in the number of patient safety publications and editorials on both human and veterinary anaesthesia. Awareness is being raised through promotion of ‘safe’ anaesthesia practice by the AVA and supported by the continuing professional development given by many of its members. With this ‘starter kit’ the tools are available to allow each and every veterinary practice to make a change. However, it will need the support of all members of the veterinary professions caring for patients in a peri-operative environment to put this patient safety driven initiative into practice and make a difference (Staender et al, 2013). While the profession is some way from having a UK central adverse event and critical incident reporting system for anaesthesia, this is something that the profession should be striving to achieve in order to significantly improve patient standards. To paraphrase Hogan and Sanders (2014): ‘we can only hope that when future generations look back and describe the development of veterinary anaesthesia that one of the key themes from our time will be the formalised importance of learning from our errors’.
