
Brachycephalic breeds have arisen due to the human population breeding from animals that have local chondrodysplasia, and at present no specific genes have been identified (Bofan et al, 2015). Due to selective breeding these animals now present with common set of anatomical attributes including stenotic nares, hypoplastic trachea, an elongated soft palate and everted laryngeal saccules. This results in the airway being impaired and, alongside the high prevalence of regurgitation in these animals, this can result in aspiration pneumonia as a secondary disease. In extreme cases patients may also present with laryngeal collapse. The most commonly reported signs by owners include reduced exercise tolerance, stridor, coughing, respiratory distress, panting excessively and in extreme circumstances collapse (Furtado, 2014). Animals presenting with brachycephalic obstructive airway syndrome (BOAS) in practice will show other clinical signs including stertor accompanied with inspiratory dyspnoea, syncope, cyanosis, snoring, gagging and gastrointestinal signs including vomiting, regurgitation and dysphagia (Furtado, 2014). Airway obstruction may be the most commonly noticeable disease of these breeds, but there are other diseases that have been created by breeding animals in this way. They may be at an increased risk of corneal ulceration and globe prolapse, dental overcrowding and malocclusion, the excess of skin folds can cause pyoderma and a vertebral anomaly known as hemi vertebra, which is the lack of formation of one half of the vertebral body, which can result in spinal cord compression (Ladlow, 2018). The treatment for BOAS is surgical intervention, which may include shortening of the soft palate (staphylectomy), tonsil resection, removal of everted laryngeal saccules, nostril resection and laser assisted turbinectomy.
Informed consent
Many clients will be unaware of the extent that BOAS is effecting their pet. Some important questions to ask on admission include: respiratory noise at rest and when playing/exercising; how active they are; do they pant often; exercise tolerance; changes in activity in hot weather; any noise when sleeping; and any episodes of fainting or collapse. With the last question it is important to consider that owners may not see their dog frequently stopping mid walk as a problem, and additional questions may be required to get all the history needed. As with any anaesthetic the consent form must be completed prior to the procedure being carried out. These patients are extremely high risk and therefore it is important that the owner is made aware and fully informed of the options available, risks of the procedure and anaesthetic, and given an estimate of costs so they can provide fully informed consent.
Premedication
Prior to any medication, bloods for biochemistry and haematology should be taken if indicated and an intravenous (IV) catheter placed. If an IV catheter cannot be placed due to the patient becoming stressed and having respiratory difficulties, then a premedication can be given intramuscularly (IM); although IM premedications are routine in practice, with these patients IV access is ideally obtained before any sedative/opioid combination is given so the patient can be anaesthetised immediately if the airway becomes compromised. Once this medication has been given it is vital to monitor this patient in a one on one setting, and provide oxygen supplementation. All materials needed for the placement of an IV catheter should be on hand, as well as the materials required for anaesthetic induction, intubation and anaesthetic maintenance (Figure 1); an additional item that may be used is a spay hook which can assist in assessing the length of the soft palate. There are a variety of premedications available to use in practice and a large number of combinations that can be used for brachycephalic patients. The author's practice uses a combination of a phenothiazine, acepromazine (ACP, Novartis Animal Health) and a full agonist opioid methadone (Comfortan, Dechra). The dosage of ACP that is used is the lower end of the range (0.005 mg/kg), and methadone is used at a dose of 0.2 mg/kg. It could be argued that ACP should not be used as it cannot be reversed, therefore a better alternative would be dexmedetomidine (Dexdomitor, Zoetis), which is an alpha 2 agonist and can be reversed using atipamazole (Antisedan, Zoetis). One disadvantage of this drug is that brachycephalic breeds have a high vagal tone; alpha 2 agonists increase the vagal tone further resulting in bradycardia. The advantages of using ACP is that it provides anxiolysis, sedation, is an antiemetic (a consideration in a breed which presents commonly with gastrointestinal signs), and has minimal effect on heart rate following vasodilation, which increases cardiac output (Blazquez and Vettorato, 2018). Multimodal analgesia may be used with a combination such as methadone (Comfortan, Dechra) and a non-steroidal anti-inflammatory (NSAID) such as meloxicam (Metacam, Boehringer Ingelheim). On the other hand some surgeons prefer to use steroids in the pre-operative period to reduce any oedema, for example dexamethasone (Dexafort, MSD) 1 mg/kg IV (Furtado, 2014).

Gastro-oesophageal reflux (GOR)/regurgitation
Brachycephalic breeds are at an increased risk of GOR or regurgitation when under anaesthesia, and regurgitation is easier to see as the fluid is expelled through the mouth or nose whereas reflux remains within the oesophagus. It has been reported that the length of time a patient is starved can affect the occurrence of GOR. Historically patients were starved for a period of 12 hours and water made available until the premedication was administered. In veterinary medicine there is still some confusion with regards to the correct time to starve a patient before surgery. Animals starved for a shorter period of time before anaesthesia (2–4 hours) have been found to have no reflux whereas those starved for a longer period of time (12, 18 or 24 hours) have a higher incidence of reflux (O'Dwyer, 2016). It is important to inflate the endotracheal cuff as soon as the patient is anaesthetised and keep the cuff inflated in recovery until laryngeal function and consciousness has returned, however this may result in other complications (Lamata et al, 2012). Due to the increased risk of reflux and regurgitation in these patients, a proton pump inhibitor such as omeprazole, which has been shown to lower the incidence of GOR, can be used at a dose of 1 mg/kg pre-emptively (Panti et al, 2009). While omeprazole can be used preoperatively to prevent vomiting and regurgitation, some recommend using metoclopramide (Emeprid, Ceva) as an alternative (Trappler and Moore, 2011).
Oxygen supplementation
Prior to anaesthetising the patient it is recommended to provide oxygen supplementation for a period of 3–5 minutes, and in brachycephalic patients whose oxygen saturation will already be below the average of 95% on room air, it is important to provide a higher percentage of oxygen in the functional residual capacity of the lungs, which will delay oxygen de-saturation (McNally et al, 2009, Adshead, 2014). There are a variety of methods available to do this and the most common and easiest method is using a mask (Figure 2). If the patient will not tolerate this then the mask can be removed and flow-by oxygen provided by the anaesthetic circuit. One study conducted by Ambros et al (2018) evaluated the use of pre-oxygenation provided by either mask or flow-by methods for a period of 3 minutes prior to induction. They found that providing oxygen to the patient for 3 minutes by mask provided a longer time to desaturation compared with the flow-by technique. When using a mask it is important to be aware of the patient's eyes and the position of the mask so as not to cause damage or irritation to the outer eye, as these breeds have decreased corneal sensitivity. Brachycephalic breeds' protruding eyes makes them more susceptible to ocular disease than other breeds, and several writers have investigated the prevalence of certain health problems other than BOAS in these animals. They found that they were three to four times more likely to have corneal ulcers and conjunctivitis (Gyles, 2017). Other methods of oxygen supplementation include nasal prongs, however in patients that have stenotic nares it can be difficult to fit them correctly and they may cause more stress to the patient.

Induction and intubation
A propofol (Propoflo Plus, Abbott) or alfaxalone (Alfaxan, Jurox, UK) induction is used intravenously to effect, if either of these induction agents is administered too rapidly then there is a risk of respiratory depression and apnoea. In patients that already have an occluded upper airway, this can be detrimental alongside a difficult intubation (Adshead, 2014). A laryngoscope must always be used to aid intubation, which can be hindered due to the anatomical problems associated with this breed, and a smaller endotracheal tube (ET) is required to intubate, sometimes known as a rescue tube. Intubating a brachycephalic animal can be difficult; one method to combat this is to have a urinary catheter available that can be placed into the trachea as a guide, the endotracheal tube can then be guided over the urinary catheter into the airway and the catheter removed. Armoured ET tubes may be used and can be very useful in preventing the ET tube from kinking during diagnostics and surgery; however they cannot be used in computed tomography (CT). If correct placement of the ET tube is under question then capnography can be very useful in checking the tube is in position.
Diagnostics
Part of the preoperative assessment of these patients includes thoracic radiography, this allows for assessment of the trachea and lungs, which is important due to the prevalence of reflux and regurgitation in these breeds. This can in turn result in aspiration pneumonia which cannot always be diagnosed on lung auscultation (Shales, 2014). One of the components of BOAS is a hypoplastic trachea, this involves a growth abnormality in the tracheal cartilage rings resulting in a narrowed airway, and thoracic radiography can assist in the diagnosis of this condition. A flexible scope may be required alongside radiography to assess the trachea and rigid scope to check the nasal turbinates; however another consideration for these patients is that they are at an increased risk of having a hiatal hernia which cannot always be seen on radiography. The gold standard for assessing these patients pre-operatively is CT; this allows for assessment of the nasal turbinates, soft palate thickness and thorax, therefore detecting a hiatal hernia. However, use of CT is dependent on the finances available and it is acceptable to carry out surgical treatment based on clinical examination alone (Ladlow, 2018).
Surgical preparation
There is minimal surgical preparation for these cases in terms of removing hair or using a surgical scrub; an oral mouth rinse is used to lower the bacterial levels prior to surgery, and the nose and nasal folds cleaned using dilute chlorhexidine or povidone iodine. Theatre preparation is different for every case and these animals will be positioned in sternal recumbency with their heads elevated and mouth open. The easiest way to achieve this is to use two drip stands and place one either side at the end of the operating table. The lower jaw can then be secured using tape and the upper jaw held open using tape between the two drip stands (Figure 3).

Anaesthetic monitoring
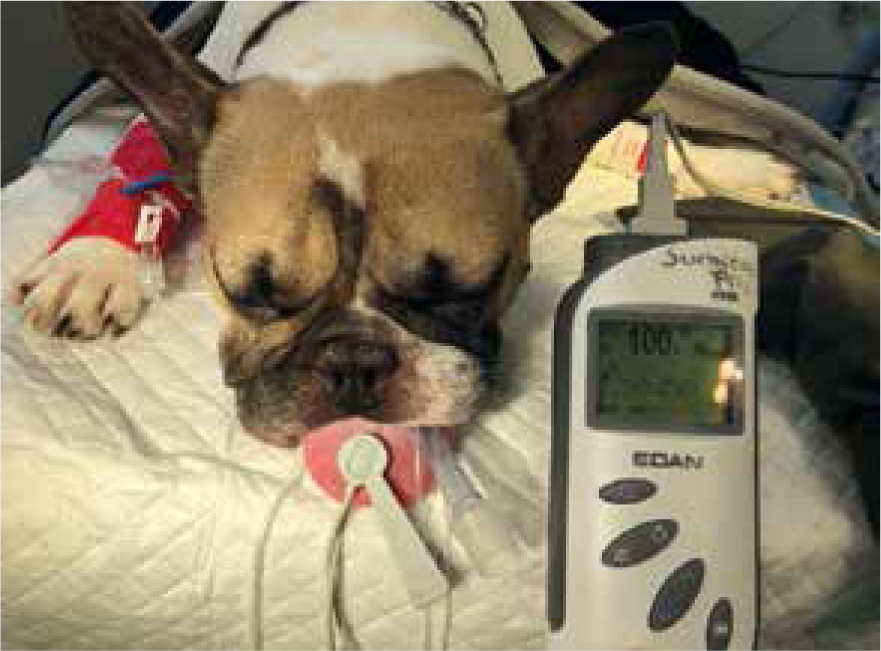
Once these patients are intubated and the airway protected the anaesthetic monitoring is the same as for any other anaesthetised patient. The patient's temperature, heart rate, pulse rate, respiration rate, capillary refill time and eye position (which may be obscured by drapes or if the surgeon tapes the eyes closed to prevent damage to the globes) are monitored throughout, the positioning of the patient for the procedure makes it impossible to monitor the jaw tone. Monitoring the oxygen saturation is vital and it should remain above 98%. If it drops any lower intermittent positive pressure ventilation (IPPV) is required to increase it back to within the normal range. Hypoventilation can be a problem for patients under anaesthesia due to the depression of the respiratory system because of the anaesthetic agents used. As the patients are intubated with a smaller ET tube due to the already narrowed airway, the area for gas exchange is at a high resistance (Adshead, 2014). The end tidal carbon dioxide (CO2) should remain between 35–45 mmHg, however it is important to remember that these patients may have hypercapnia before being ventilated, and therefore their CO2 levels may be higher than normal initially. In the author's experience these patients can hyperventilate and therefore have hypocapnia under anaesthetic. Both hypocapnia and hypercapnia can be resolved either by using manual ventilation (IPPV) or using a mechanical ventilator if there is one available in the practice. IV fluid therapy is provided, guidelines used to recommend surgical intravenous fluid therapy rates to be 10 ml/kg/hour, however with more evidence in both human and veterinary medicine, it is now stated to administer a starting dose of 3 ml/kg/hour in cats and 5 ml/kg/hour in dogs (Robinson, 2016). Blood pressure can be monitored using a variety of techniques including Doppler, oscillometric or arterial, this is dependent on what is available in practice. If the mean blood pressure goes below 60 mmHg then a bolus of crystalloid fluid should be given; in practice the author uses a rate of 10 ml/kg over 15–20 minutes until normalised. As stated earlier, these patients are at a high risk of ophthalmic problems due to the bulging eyes, therefore lubricant should be used and applied frequently throughout the anaesthetic or the eyes should be taped closed.
Surgical process
As stated earlier BOAS consists of multiple anatomical problems, some of which are not identifiable until the patient has been anaesthetised. From looking at the patient the veterinary surgeon will be able to decide if the nares require surgery, however viewing the laryngeal saccules, soft palate and tonsils will only be possible on induction. The elongation of the soft palate causes obstruction into the opening of the airway (larynx) and interferes with the movement of air into the lungs during respiration. A staphylectomy (full thickness resection) is performed to shorten the soft palate; care must be taken not to shorten the soft palate excessively as this can cause sinusitis, rhinitis and aspiration (Trappler and Moore., 2011). A newer alternative technique is called a folding flap palatoplasty which involves making the soft palate thinner and shorter by removing a portion of the oropharyngeal mucosa, and made shorter by folding it on itself (Bofan et, al, 2015). The veterinary surgeon's preference will dictate whether the soft palate is shortened using sharp dissection, a carbon dioxide laser or vessel sealing device (Figure 4). The advantages of using a carbon dioxide laser or vessel sealer include minimal haemorrhage, a shorter surgical time, decreased swelling and postoperative pain (Lodato and Mauterer, 2014). The next procedure is to remove the laryngeal saccules which are positioned between the lateral wall of the larynx and vocal folds. In normocephalic breeds they do not cause a problem, but in brachycephalic patients they can become everted and obstruct the airway. There is some debate in the literature as to whether removing the saccules has a beneficial effect in improving air flow. One study by Cantatore et al (2012) performed a unilateral sacculectomy in 10 dogs, the results showed that none of the laryngeal saccules spontaneously resolved and that resection resulted in an 80–90% increase in airflow. This study also found that in one dog after a sacculectomy there was proliferation of a soft tissue lesion, which was endoscopically similar to a newly formed saccule. From a nurse's perspective laryngeal saccule resection involves extubating the patient during surgery to allow access and visualisation for the surgeon, therefore the patient's anaesthetic plane is maintained via a total intravenous anaesthesia (TIVA) using propofol (Propoflo Plus, Abbott) or alfaxalone (Alfaxan, Jurox, UK), and oxygen supplementation until the patient can be intubated again. Another procedure that can be performed is tonsil resection; this is also a controversial area among surgeons. Some would argue that the effect the tonsils have on air flow is minimal and the result in a controlled condition (anaesthetised patient) differs from that of a conscious patient. This is due to changes in the air flow, such as negative pressure and turbulence, therefore it is performed to try and maximise the surgical benefit (Shales, 2014). Once the soft palate surgery, laryngeal saccule and tonsil resection have been performed the patient's upper jaw can be removed from suspension ready for surgical correction of the nares. There are a variety of surgical techniques available including wedge recession, laser ablation, alar wing amputation (Trader's technique), and alapexy for the correction of stenotic nares (Figure 5). Regardless of what technique is used early correction of stenotic nares is recommended to prevent the progression of BOAS and improve prognosis (Trappler and Moore., 2011). A newer technique that addresses the nasal obstruction in these animals is a laser assisted turbinectomy (LATE); this can be used when patients have had minimal response to conventional surgery and are still clinically affected by the condition. When LATE is performed in patients that have had minimal response to conventional surgery a further 80% are said to be clinically unaffected after (Ladlow, 2018).




Recovery
The main post-surgical complications in these patients include airway swelling, vomiting, regurgitation and aspiration pneumonia (Trappler and Moore, 2011). During the anaesthetic the patient's airway is maintained and protected by the ET, therefore extubating these patients is an extremely high risk period. Extubating too early can result in upper airway obstruction therefore it is recommended to leave the ET tube in for a longer period of time, most will be in sternal recumbency, awake and head lifting with the tube still in position with no adverse effects, and the oxygen saturation remaining within normal limits (Figure 6). When the patient is extubated it is important to provide postoperative oxygen supplementation via mask and recover these patients next to an anaesthetic machine with all the materials required for intubation and induction available. Postoperative positioning is also important, as stated earlier these patients are at a high risk of GOR which can occur in recovery, therefore it is advisable to position them in sternal recumbency with their head elevated. A helpful aid to recovery is having a suction machine, tubing and suction tip available if there is any regurgitation so it can be quickly removed before aspiration.
Tear production is said to be decreased after the anaesthetic period; one study by Komnenou et al (2013) found that animals had a decreased tear production up to 2 hours post general anaesthesia and recommended the use of tear substitute treatment in this time frame. It is advisable to lubricate the eyes every 30 minutes for 2 hours post anaesthesia to prevent corneal ulceration.
BOAS surgery can cause inflammation and due to the position of the surgery in these patients, the author's practice withholds food until the day after surgery, however other practices may feed these patients the same day. Once assessed by the veterinary surgeon the next day, a small amount of wet food should be offered and the patient monitored for any adverse effects including change in respiration rate and effort and vomiting.
Post-operative care
There are many aspects in the postoperative period that need to be considered for these patients, and as all cases are hospitalised for at least 24 hours post surgery, recovery needs to be as calm and stress free as possible. Dogs do not sweat like humans therefore they use panting as a way to get rid of excess body heat and thermoregulate. Patients that have undergone BOAS surgery should be kept within a normal temperature range whether this includes the use of a fan, cool mat or airconditioning in recovery to prevent excessive panting. To keep the patients calm and stress free, you can use a pheromone diffuser such as dog appeasing pheromone (DAP) (Adaptil, CEVA) in the kennel area. Keep the patient away from vocal inpatients, and in some cases it may be necessary to allow the patient to be discharged the same day, if the patient is anxious to the point where it may have a negative impact on recovery. The aim is to provide a smooth and stress free recovery for any patients undergoing anaesthesia, however some animals, especially brachycephalics, may need sedation to assist with a stress free recovery. Dexmedetomidine (Dexdomitor, Zoetis) can be used in these patients at low doses of 0.5–1 μg/kg IV. By providing the correct care to the patients in recovery it is possible to prevent an ever increasing respiratory rate, which can result in dyspnoea, hypercapnia, worsening obstruction of the airway, decreased heat loss and hyperthermia, all of which are contributing factors to upper respiratory collapse (Blazquez and Vettorato, 2018).
Home management
Due to the location of the surgery it is important that no pressure is put on the neck, and patients should be discharged with a harness and kept in a cool environment. Exercise is also restricted during recovery to two 5–10 minute lead walks twice a day for a period of 6 weeks; after this exercise can gradually be increased by 5 minutes each week until the final postoperative check. The patient is seen 2 and 10 days after surgery to monitor their progress, and earlier if there are any complications or concerns. Wet but solid food is fed for a period of 6 weeks to minimise airway irritation before they are transitioned onto dry food if that is their normal diet. Owners need to be informed that the patient needs to be walked during the cooler times of the day (morning and night), kept in cooler areas of the house (away from conservatories in the heat), and to provide a fan if needed. Client education is vitally important in these patients and assists with a positive outcome from surgery.
Conclusion
The anatomical differences of brachycephalic patients are well documented in veterinary literature and with the increased popularity of these breeds, higher numbers are being seen in practice. From admission to discharge these patients have specific needs and anaesthetic protocols and nursing care should be adjusted accordingly.