Upper respiratory tract (URT) surgery is common in equine practice. Horses with URT issues often present to the clinic with a history of poor performance or the presence of an abnormal respiratory noise (whistle/roar/gurgle) during exercise.
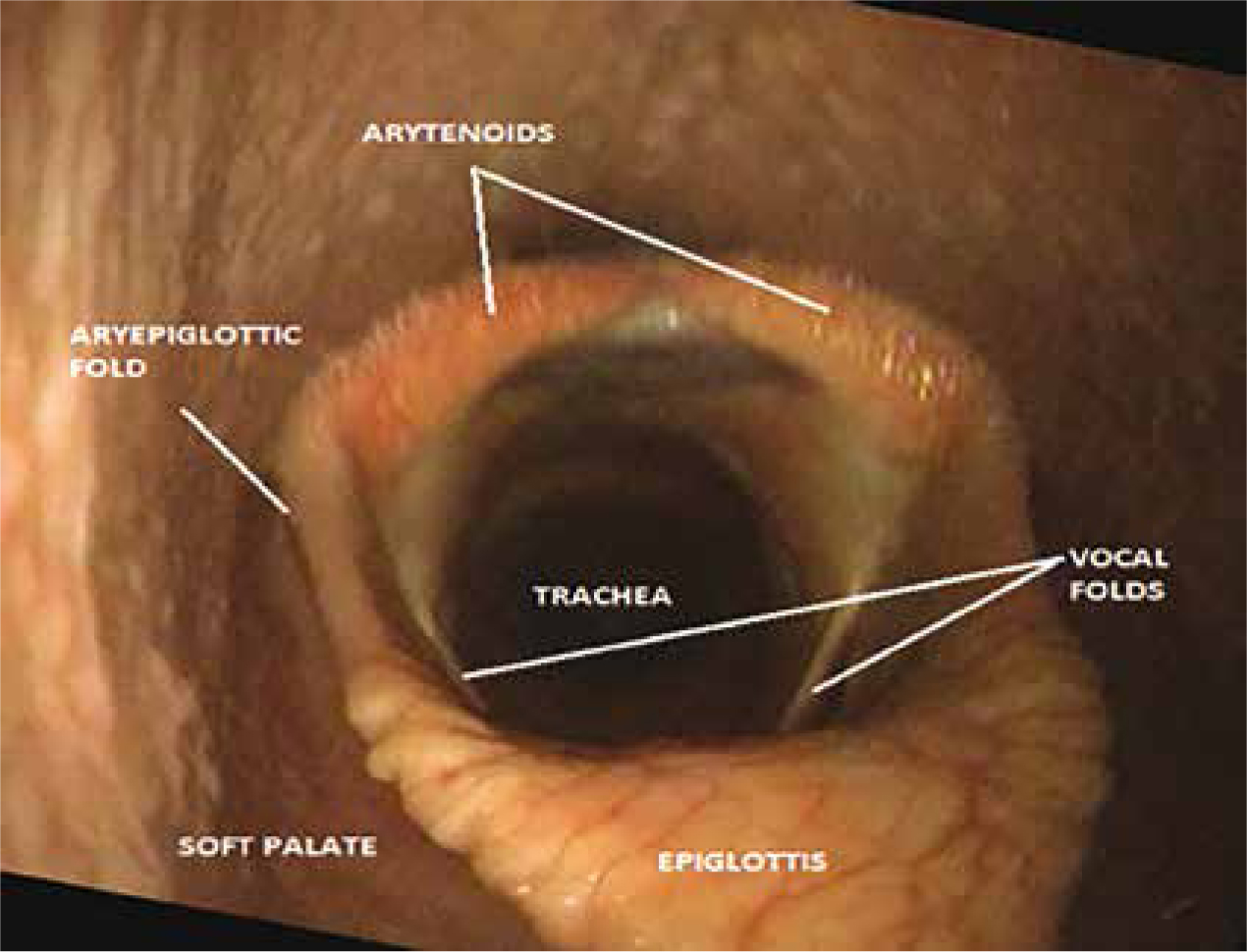
In working up these cases, a full history is obtained, a comprehensive physical examination is performed with particular attention given to the upper portion of the respiratory tract, and standing/resting endoscopy or overground endoscopy (OGE) is performed. Figure 1 is an image of a normal larynx at exercise. In some cases, abnormalities, e.g. subepiglottic cysts, can be diagnosed by resting endoscopy, but further assessment of complex abnormalities by OGE allows the veterinary surgeon (VS) to assess the function of the pharynx and larynx while the horse is under strenuous exercise (Barnett et al, 2015).
The common URT surgeries discussed in this article are
A brief description of the pathology that requires surgical correction will be discussed, surgery details that the nurse needs to be aware of, and the postoperative care required for each surgery.
Routine patient preparation for airway surgery
It is common practice to starve the patient for 8 hours prior to surgery if the patient is to undergo a general anaesthetic (King, 2014).
The intravenous catheter (IVC) should be placed lower down on the jugular than the normal position of the first one third of the neck as the surgical site is near the top of the neck; or if appropriate the IVC can be placed in the opposite jugular. Pre-medications should be administerd as prescribed by the VS in charge. This may include analgesia, sedatives and antimicrobials.
Routine postoperative protocols
It is advisable to keep a tracheostomy kit at the patient's stable for 3 days postoperatively as laryngeal oedema can develop very quickly post surgery, which can lead to obstruction of the airway. Table 1 contains a list of equipment needed for an emergency tracheostomy.
| Tracheostomy tube | Gauze swabs soaked in 4% chlorhexidine scrub solution |
| Clippers | Gauze swabs soaked in surgical spirit |
| Sterile gloves | No. 10 scalpel blade |
| Local anaesthetic (e.g. mepivacaine hydrochloride 2%) 5–10 ml drawn up in syringe with 23/25 G needle labelled | Suture material |
Postoperative feeding is different for each particular surgery; to ensure all members of the team are aware of this, it is advisable that a sign stating whether the patient is to be fed and watered from the floor or from a height, be placed on the patient's door.
Prosthetic laryngoplasty (tie back)
Indications
Prosthetic laryngoplasty is used to treat horses suffering from recurrent laryngeal neuropathy (RLN) or laryngeal paralysis. RLN is a condition of the larynx that results in the inability of the horse to successfully abduct the arytenoid cartilage. This subsequently causes a reduction in airflow to the lungs and in turn exercise intolerance.
RLN can be a progressive disease and may present as unilateral or bilateral paralysis, but the left arytenoid cartilage (Figure 2) is most commonly affected (Biasutti et al, 2016).

Diagnosis of RLN is based on history including exercise intolerance, noise at exercise and full physical examination. The ‘gold’ standard for accurate diagnosis is OGE at exercise.
Surgery notes
This surgery is performed under general anaesthesia with the patient in lateral recumbency, affected side up with head and neck extended. Prosthetic laryngoplasty is the placement of a prosthesis, i.e. a suture through the paralysed arytenoid cartilage which is ‘tied back’ into an open/abducted position. This procedure is usually done in conjunction with a ventriculocordectomy so the horse's position is changed to dorsal recumbency once the prosthetic laryngoplasty is complete. The ventriculocordectomy should provide a larger airway diameter and additional fibrosis for support of the arytenoid cartilage in an abducted position and to minimise noise production (Brown et al, 2004).
This procedure can also be performed in the standing sedated horse. The advantages of standing prosthetic laryngoplasty are: it avoids the risk of general anaesthesia, reduces costs, and allows the accurate intra-operative abduction of the arytenoid cartilage (Rossignol et al, 2015).
Postoperative care
The horse is fed and watered from the ground for the rest of its life (Biasutti et al, 2016). This is to reduce the risk of the aspiration of food and water.
The horse is box rested for 4 weeks. They may be hand walked during the second postoperative week; 30–45 days post operation the horse can be exercised lightly. Full training should not be resumed for at least 2 months post operatively (Kidd and Slone, 2002).
Postoperative complications include: the prosthesis failing to maintain abduction; coughing; nasal discharge; dysphagia; aspiration pneumonia; chrondritis and laryngeal oedema. In one study, it was reported that 2.5% of horses can be expected to be left with a chronic cough while eating (Kidd and Slone, 2002) .
Ventriculocordectomy (Hobday)
Indications
This surgery is used to reduce noise in race/sport/draught horses. Horses producing this noise are sometimes referred to as ‘roarers’. As this surgery does not produce any abduction of the arytenoid cartilage, it is not recommended as a sole procedure for horses affected with advanced RLN. This surgery is often done in conjunction with a prosthetic laryngoplasty.
Diagnosis is based on history and OGE to rule out other causes of respiratory noise.
Surgery notes
The horse should be positioned in dorsal recumbency. The surgery is performed via laryngotomy therefore the area between the ventral jaw is clipped and aseptically prepared (Figure 3).

Postoperative care
The incision needs to be cleaned twice a day with saline soaked swabs. It is not advisable to use an antimicrobial skin cleaner as if it too concentrated it becomes toxic to the cells involved in wound healing (Pritchard, 2015). Petroleum jelly may be applied around the incision site to protect the surrounding skin from the discharge.
These patients are fed and watered from the floor. The horse is then box rested for 2 weeks, followed by walking exercise for 3 weeks before recommencing normal training.
Laryngeal tie forward
Indications
This procedure is used to correct intermittent dorsal displacement of the soft palate (IDDSP).
IDDSP is when the caudal border of the soft palate becomes displaced to a position dorsal to the epiglottis (Allen, 2015). This obstructs the opening to the trachea and in turn reduces the amount of air the horse can expire (Figure 4). This becomes an issue when the horse is at exercise (Franklin et al, 2002).

Horses with IDDSP usually present with a history of abnormal expiratory noise and exercise intolerance during strenuous training. The abnormal noise has been described as a rattling, gurgling or snoring principally during expiration but it has been noted on both inspiration and expiration.
Diagnosis
As IDDSP is a dynamic URT disorder the best way to diagnose the condition is by OGE during exercise, which is usually performed under ridden exercise (Allen, 2015).
Surgery notes
Surgery is performed under general anaesthesia and the patient is positioned in dorsal recumbency with the neck straight and extended. A midline incision is made on the ventral cervical area. The site clipped and aseptically prepared.
This procedure involves permanently fixing the larynx forward by means of two sutures (Polyester Suture/FiberWire suture, ETHIBOND EXCEL®, Ethicon) placed either side of the larynx tied to the more rostrally positioned basihyoid bone.
Postoperative care
Monitor incision for heat, swelling and discharge. The patient is fed and watered at shoulder height for the rest of its life. As this procedure involves suturing the larynx into a more rostral position, feeding the patient from shoulder height prevents putting unnecessary strain on these sutures.
The horse is box rested for 2 weeks, followed by 2 weeks of walking exercise prior to gradual introduction to normal training.
Surgical excision of epiglottic entrapment
Indications
Epiglottic entrapment occurs when the aryepiglottic folds and subepiglottic mucous membranes envelop the epiglottis (Figure 5). Ulceration of the entrapping mucous membranes over the epiglottis may occur in some cases.

The majority of affected horses produce an abnormal respiratory noise at work and display exercise intolerance. Less frequent clinical signs are coughing and nasal discharge. In some horses epiglottic entrapment is an incidental finding during endoscopy for another reason (Coleridge, 2015).
Diagnosis is based on history and endoscopic examination.
Surgery notes
This procedure is most commonly performed on a standing, sedated horse under endoscope guidance. The larynx and entrapping membranes are topically anaesthetised (Auer and Stick, 2012). A long, hooked cutting instrument is placed through the mouth/nose to incise the entrapment down the midline. This procedure can also be performed with a laser. In the more unmanageable, fractious horse this procedure can be performed under general anaesthesia.
Postoperative care
Horses are box rested for a week. Horses with an uncomplicated recovery can return to work after 10 days' rest. Some horses also experience DDSP after this surgery which will also need correction (Coleridge et al, 2015).
Surgical excision of subepiglottic cyst
Indications
Cysts can occur in any breed but are frequently reported in Thoroughbreds. It is believed that most subepiglottic cysts are present from birth, but if not overly large, may not be discovered until the horse is mature and starts training (Salz et al, 2013). Cysts are usually a pale pink and round ,covered with mucosa and can be seen beneath the epiglottis (Figure 6).

Clinical signs of subepiglottic cysts in foals are dysphagia, aspiration pneumonia and airway obstruction. In older horses cysts can present with nasal discharge, dysphagia if the cyst is large, poor performance and abnormal respiratory sounds during exercise.
Diagnosis
Endoscopy is used to diagnose subepiglottic cysts. Radiographs can also be taken to get more information on location and size.
Surgery notes
Postoperative care
The laryngotomy site is cleaned twice daily and petroleum jelly is applied around the surrounding skin to protect from discharge. The horse is returned to training 4 to 6 weeks post operatively if the area has healed normally and the follow up endoscope is normal.
Partial arytenoidectomy
Indications
Partial arytenoidectomy is performed on horses suffering from arytenoid chrondritis (abnormal enlargement of one or both arytenoid cartilage) (Figure 7) or horses with RLN/laryngeal hemiplegia where previous laryngoplasty surgery has failed; causes of this failure can include trauma or infection. It involves the surgical removal of the affected arytenoid cartilage (Barnes et al, 2004).




Diagnosis is based on history, clinical examination and endoscopic examination of the larynx. Ultrasound can be used to visualise the different appearance of the affected cartilages. Palpation of the larynx may also demonstrate asymmetric musculature.
Surgery notes
The treatment depends on the presentation of the disease, that is whether it was acute or chronic, the amount of airway dysfunction and the level of athletic activity the horse is required to do.
The horse is anaesthetised, positioned in dorsal recumbency and a laryngotomy is performed. A tracheotomy tube is place mid-neck; the tracheotomy tube may be placed before or after the induction of anaesthesia. In the author's clinic it is placed in the induction box with the horse sedated prior to being induced.
It is advisable to sterilely prepare adrenaline-soaked swabs for this procedure to help control intra-operative haemorrhage (White and Blackwell, 1980).
Postoperative care
The laryngotomy incision site is cleaned twice daily. The tracheotomy tube should be removed and cleaned daily. The tube is left in place until the airway patency is confirmed.
Depending on the case or clinician, food may be withheld for the first 24 hours post operatively or re-introduced sooner. When food is re-introduced it is fed from the ground. Feed wet hay and sloppy mashes until the horse is able to eat without coughing. Turning the patient out to grass in a small pasture is recommended (Parente et al, 2008)
The horse is box rested for 4–6 weeks, this is followed by walking exercise for a further 4–6 weeks before the horse can return to work if the surgical site has healed and no complications have occurred.
Postoperative complications can include coughing (which can continue for months before ceasing), dyspnoea, dysphagia and laryngeal oedema (Davidson and Parente, 2011).
Resection of the aryepiglottic folds
Indications
Resection of the aryepiglottic folds is indicated in cases with medial deviation of the aryepiglottic folds (MDAF) which may cause dynamic partial upper airway obstruction during exercise. Affected horses are generally young (<3 years) and present with a history of exercise intolerance and abnormal inspiratory noise (Hawkins, 2015).
Diagnosis is made during OGE at exercise because the collapse of the aryepiglottic folds only occur at high speed exercise.
Surgery notes
Postoperative care
The horse is boxed rested and walked in hand for 2–3 weeks before returning to full exercise (King et al, 2001).
Conclusion
A good understanding from the nursing team of the different pathologies of the upper respiratory tract, how they are diagnosed and surgical techniques is important to appropriately prepare the patient for surgery, to set up the operating room accordingly, and to properly manage the patient post operatively. A summary of the common URT sugeries is provided in Table 2.
| Surgery | Disorder | Surgery notes | Post-operative care |
|---|---|---|---|
| Ventriculocordectomy (Hobday) | To treat ‘roarers’ | General anaesthetic (GA)/dorsal recumbency | Incision site is cleaned |
| Prosthetic laryngoplasty (tie back) | Recurrent laryngeal neuropathy (RLN) or laryngeal paralysis | GA/lateral recumbency or Standing sedated | Incision is cleaned twice daily |
| Laryneal tie forward | To correct dorsal displacement of the soft palate (DDSP) | GA/dorsal recumbency | Monitor incision for heat, swelling and discharge. |
| Surgical excision of epiglottic entrapment | Epiglottic entrapment | Standing, sedated horse endoscopically guided | Box rest for a week |
| Excision of subepiglottic cyst | Subepiglottic cyst | GA/dorsal recumbency or lateral recumbency or standing sedated | Incision site is cleaned twice daily |
| Arytenoidectomy | To treat arytenoid chrondritis or horses with RLN where previous surgery has failed | GA/dorsal recumbency | Incision site is cleaned twice daily |
| Resection of the aryepiglottic folds | Indicated in cases with aryepiglottic fold collapse | GA Or standing sedated | Box rested and walked in hand for 2–3 weeks |