Anorexia is a common condition in cats, usually associated with an underlying illness. If anorexic conditions are not rectified, complications such as gastrointestinal atrophy, compromised immune system and delayed tissue repair are likely to develop (Chan, 2009). Manual feeding techniques such as the use of strong smelling, warm and moist food, hand feeding or feeding the diet fed at home should be attempted primarily, unless there are gastrointestinal complications, physical disabilities or the patient requires immediate nutritional support for survival. Appetite stimulants should only be used as a last resort as they do not have long-term benefits (Delaney, 2006).
This investigation analyzed the effect of feeding the diet fed at home, strong smelling, moist and warmed food, or hand feeding to encourage voluntary food intake in anorexic cats while hospitalized in the veterinary environment. This investigation considers manual feeding methods in more detail, with a view to presenting information on the most effective methods of encouraging food intake to ensure that anorexic cats are provided with simple, effective nu-tritional support. This will encourage a quick return to voluntary intake, thus minimizing complications and reducing recovery time.
Literature review
Olfaction and gustation: effect on voluntary intake
Olfaction and gustation are used in the detection, identification and selection of foodstuffs (Bradshaw, 1991; Case, 2003). Cats appear to be able to regulate food intake (Bradshaw et al, 1996). It has been found that in humans the brain regulates food intake as ‘when one is hungry food tastes pleasant’, but if overfeeding occurs then the taste is no longer as strong or enjoyable and therefore voluntary intake decreases (Rolls, 2005), therefore use of extremely palatable and digestible foods can encourage voluntary intake (Zoran, 2008). Cats may have a strong preference for familiar foods or become neophobic and refuse to eat foods never previously encountered (Bradshaw et al, 2000).
Anorexia
Anorexia is defined as the loss of or lack of appetite (Simpson and Busby, 2003), which is often a common symptom of underlying conditions (renal failure, hepatic problems, neoplasia) in cats (Sturgess, 2003). Nutritional support is essential prior to deterioration in the patient's condition. Feline patients who require immediate nutritional support are those who have not eaten to satisfy their caloric requirements for a minimum of 3 days or have had recent weight loss of more than 10% of their bodyweight (Chan, 2010).
Malnutrition and energy and protein losses lead to a variety of complications, such as a compromised immune system, reduced tissue repair and gastrointestinal effects such as villous atrophy and decreased gut motility (Remillard et al, 2010). Recovery from underlying diseases is also severely compromised (Tennant, 2006).
Nutritional support must be implemented gradually to avoid re-feeding syndrome, which may occur after feeding carbohydrates post anorexia as a result of electrolyte and insulin imbalances (Michel, 2004; Chan, 2009), and may result in respiratory distress, heart failure and gut upset resulting in nausea or diarrhoea. Drugs such as antibiotics, non-steroidal anti-inflammatory drugs, analgesics, anti-emetics and appetite stimulants may lead to a reduction in voluntary food intake (Michel, 2001).
Enteral feeding: manual methods
Enteral nutrition, feeding the patient via the alimentary tract, is the most physiologically effective method of feeding as this preserves the role of the gastrointestinal tract (McCune and Girling, 2007). The patient must be able to hold its head in the normal position during enteral feeding, to minimize the risk of aspiration pneumonia (Remillard et al, 2010).
Increasing the palatability of food or hand feeding, should usually be the first methods to be attempted to encourage an anorexic cat to eat. (McCune and Girling, 2007; Remillard et al, 2010). These techniques should not be employed in patients with a physical disability, such as a fractured jaw where intake of food may be painful or not easily possible (Delaney, 2006).
Encouraging voluntary intake in hospitalized cats
Foods presented to anorexic cats must be highly palatable, digestible and have a high nutrient bioavaila-bility (Simpson and Busby, 2003) to ensure voluntary intake. Moisture, fat, carbohydrate and protein levels must be presented in the correct ratio and can be maintained by use of a commercially prepared diet. The Resting Energy Requirement (RER) is often used to give an approximate figure of energy requirements of the patient.
Feline hospitalization should be kept as calm and stress free as possible to maximize successful feeding (Delaney, 2006) by imitation of normal feeding patterns and cues of the time of the day. Cats appear to prefer wide, shallow ceramic or plastic bowls (Sparkes, 1993; Simpson and Busby, 2003).
Cats should be fed four to six small meals daily; overfilling the food bowl can result in a learned food aversion if the food becomes stale (Sturgess et al, 2003; Zoran, 2008). If food is not eaten in 15–20 minutes after offering, it should be removed and disposed of and the patient left without food for approximately an hour before being offered food again (Pollard and Howarth, 2006). Hand feeding by either the owner or veterinary staff not actively involved in treatment can also encourage voluntary food intake, but it can be difficult to meet caloric requirements (Burrows, 2010).
Food warmed to room temperature has been found to increase the aroma and the palatability of the foodstuf, thereby further encouraging voluntary intake (Simpson and Busby, 2003). Offering anorexic cats their usual diet may also encourage voluntary consumption of food (Bradshaw et al, 2000; Michel, 2001).
Anorexia is a common condition in cats and if nutrition is not implemented to ensure voluntary food intake, a variety of complications are likely to occur. Although general information is available as to the useful feeding techniques, there is little research into the optimal manual feeding techniques to be used. The present study aims to determine the optimal feeding technique for encouraging voluntary food intake in hospitalized, anorexic cats. The results of this investigation should aid veterinary nurses in encouraging voluntary intake by manual methods. Information may also be useful for owners, to minimize the number of anorexic cats that require hospitalization.
Materials and methods
Experimental design
The study was conducted over a year using all anorexic cats hospitalized in one veterinary practice. Anorexic cats were defined as being those which had not eaten for 2 or more days. Each cat was randomly assigned a particular feeding method in order to encourage voluntary food intake. The three feeding methods used were: hand feeding; feeding the diet fed at home; and the use of strong smelling, moist, warmed food.
A 3x3 randomized block design was used, as all cats not voluntarily eating after the first feeding method were offered the second technique, and if still not eating, the third. Each feeding technique was attempted with 20 patients, to ensure an adequate sample size to give accurate results.
Experimental routine
Patients were housed in large kennels with water available at all times. Food was offered in wide, shallow, plastic dishes. Hand feeding was attempted with palatable, easily digestible, processed food such as Hills a/d to aid voluntary deglutition. Home diets varied depending on the patient but included pouched wet food and dry biscuits. Some owners were also willing to bring in a small amount of their cat's normal diet, if this was not easily obtainable through the veterinary practice. For the third method of encouraging voluntary intake, wet, fish-based foods were warmed to body temperature prior to feeding. As necessary, patients were cleaned and groomed to remove any food that had stuck to the coat during feeding.
Food was offered an hour after hospitalization. Each feeding method was attempted for 20 minutes. If the cat ate voluntarily, this was noted as successful and the cat was no longer involved in the trial. Cats that did not eat were randomly assigned a sec-ond feeding method after a period of 1 hour with no food and were therefore counted as a second patient. Again, those cats that ate after the second method was attempted were considered successful and removed from the trial, whereas those still not eating were assigned the third feeding method. All cats in the study ate voluntarily by the end of the study. Any feeding techniques that were not successful were noted in each case. Those cats who ate voluntarily and as a result were removed from the study, were regularly monitored to ensure that adequate intake continued. Equal numbers of cats were assigned to each feeding method.
Ethics
All patients involved in the study were hospitalized for treatment within the veterinary practice. All cats were monitored closely to ensure there were no complications as a result of any feeding techniques or deterioration of their condition. Once patients were eating adequately and any underlying conditions were under control, the patients were discharged and, for the most part, were sent home with some of the food they had been eating voluntarily during the trial.
Statistical analysis
For analysis of success of feeding techniques and the numbers of cats that ate after each attempt, the chi-squared test was used. This distinguishes a significant difference between the observed and expected data according to a specific hypothesis.
Results
Effects of attempt on cats that ate
Successful voluntary intake of food in anorexic cats is essential to combat malnourishment. It can be seen from both Table 1 and Figure 1 that of the 26 cats involved in the study, all cats that were not eating voluntarily after either the first or second attempts ate successfully on the third attempt.
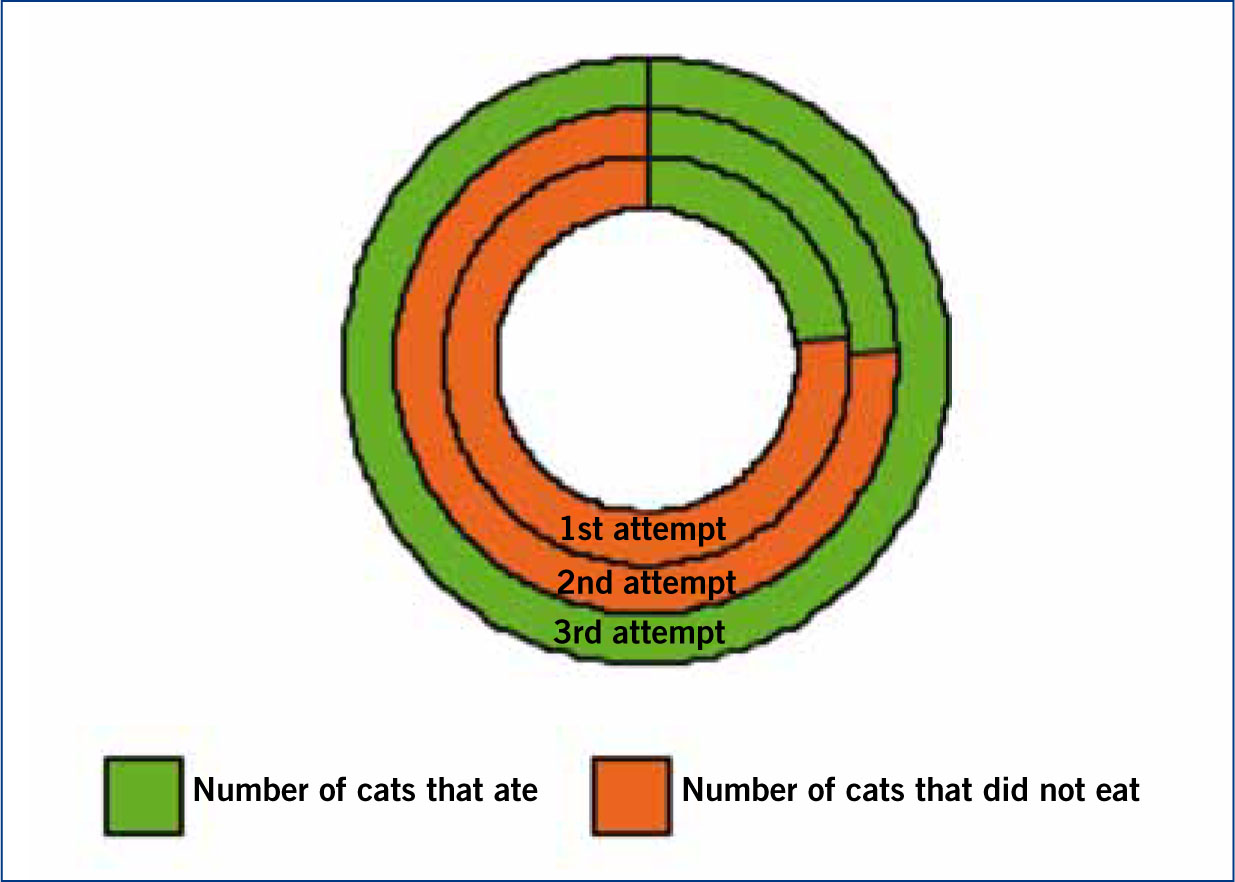
| Attempt for all feeding methods | Number of cats that ate | Number of cats that did not eat |
|---|---|---|
| 1st attempt | 6 | 20 |
| 2nd attempt | 6 | 14 |
| 3rd attempt | 14 | 0 |
A Pearson chi-squared value of 24.10 (2df) and a probability value of <0.001, under the null hypothesis, were obtained, thereby statistically supporting the significant difference in the number of cats that ate on the third attempt compared with the other two attempts (Figure 1).
Effect of feeding method on successful attempt
The study indicates there are significant differences between the feeding methods used in relation to the attempt on which the feeding method was successful (Figure 2), as a chi-squared value of 12.26 (4df) and a probability value, under the null hypothesis, of 0.016 was obtained.
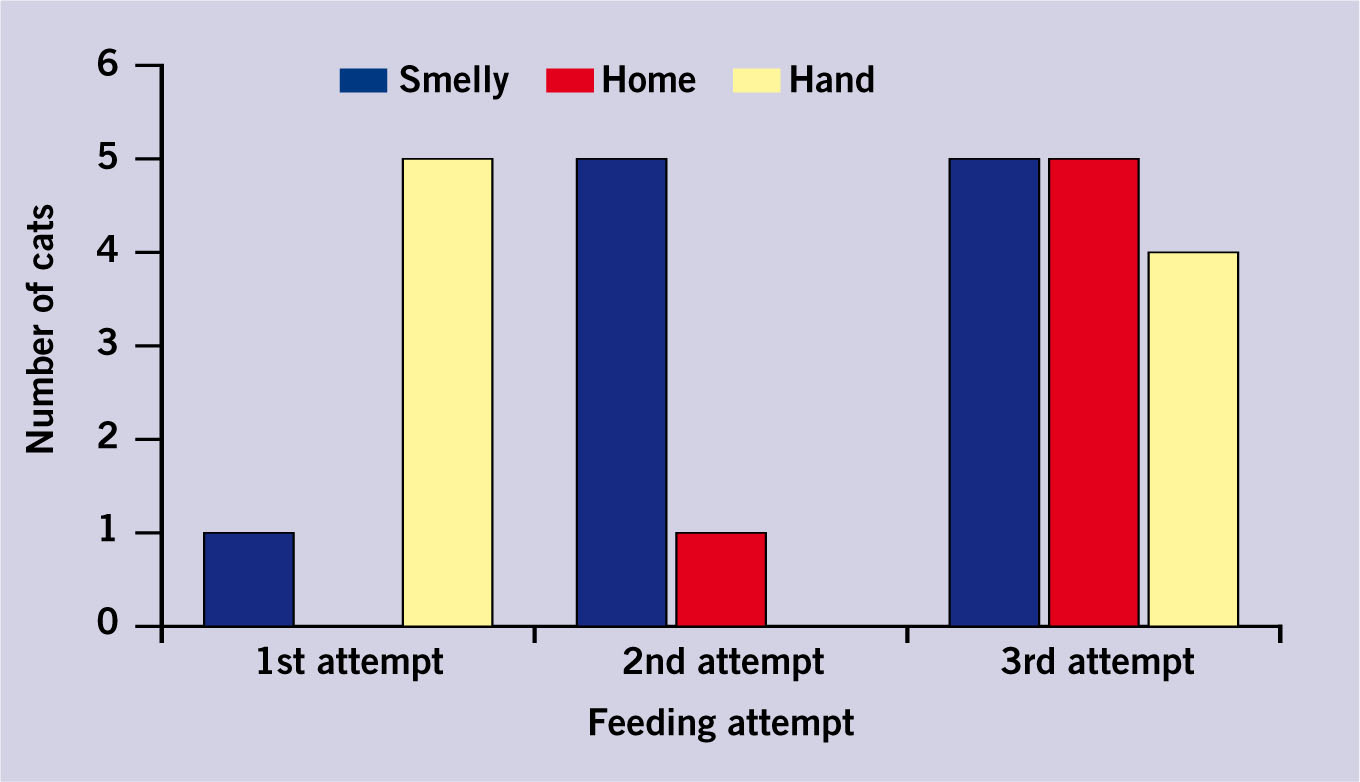
On the first attempt hand feeding was most successful, whereas on the second attempt feeding smelly, warmed, moist food was more likely to encourage voluntary intake (Figure 2). Feeding cats the diet they were usually fed at home was only successful in a few cases, mainly on the third attempt.
In addition, looking at each technique irrespective of whether it was the first, second or third attempt, 11 cats ate as a result of food being smelly and warmed, nine as a result of hand feeding, and six as a result of food being the same as that used at home. The chi-squared value indicated there was no significant difference between strong smelling food and hand feeding, but home diet was much less successful.
Discussion
Evaluation of results
The main conclusion which can be drawn from these results is that perseverance is key when attempting to encourage voluntary food intake in anorexic cats, as all cats ate on the third attempt, if not previously. This is supported by studies conducted by Sturgess (2003), in which it was found that if cats had not eaten then food should be removed and offered again after a period of time.
Results also suggest that hand feeding and feeding strong smelling, moist, warmed food can contribute towards voluntary food intake. Findings from this study confirm opinions of McCune and Girling (2007) and Remillard et al (2010), suggesting that these should be the first feeding methods attempted. Alternative techniques such as increasing the palatability of food by warming it or increasing the protein, fat or moisture content can considerably increase voluntary intake (Sparkes, 1993; Simpson and Busby, 2003; Zoran, 2008). Hand feeding has also been found to notably increase voluntary food intake in anorexic cats, but there have been worries that inadequate volumes of food are consumed if this is the only method of nutritional support implemented (Burrows, 2010). In this study all patients received adequate nutrition as a comprehensive nursing plan was developed.
From this trial, consumption of a familiar diet (i.e. one fed at home), was found to be least effective, possibly due to previous attempts to feed this diet by the owner, resulting in learned food aversions. However, although studies by Michel (2001) and Bradshaw et al (2000) showed that cats preferred familiar foodstuffs and would usually become neophobic when faced with food of unusual textures or tastes, this study has found that other manual techniques are more reliable in encouraging voluntary food intake.
Limitations
One of the main limiting factors of this study was the small sample size involved, as only inconclusive deductions could be drawn from the data collected. However, since the study was undertaken in only one small veterinary practice, the fact that 26 cats were hospitalized with anorexia during a period of 1 year shows the regularity of this condition and therefore the necessity of this research.
While chi-squared analysis was the most appropriate for the data collected, in some instances expected values were less than five and therefore the tests may have been unreliable. Again, with a larger sample this would be rectified and further significant conclusions could be made. The use of a standardized approach where all nurses carry out tasks in the same manner would allow this research to be undertaken in a variety of veterinary practices over a longer period of time and therefore an increased sample size could be attained. However, even with the best possible technique, differences between veterinary practices would need to be taken into account, whereas in this study one nurse was responsible for feeding all the cats.
Further research
In the future, further investigation into this aspect of nutritional support could be undertaken to assess the outcome of perseverance with the same feeding method versus rotation of feeding method. Further trials could also be undertaken to assess for long-term success with a combination of feeding techniques used concurrently.
Further research into the exact quantity of food eaten voluntarily could be recorded and analyzed to ensure that the patient is receiving adequate nutrition to meet its calorific requirements.
Practical implications
Anorexia is a fairly common condition seen in veterinary practice, so knowledge of the best manual methods to encourage voluntary intake is essential to ensure adequate nutritional support is implemented. It may also provide useful support for owners struggling to encourage voluntary intake in cats while suffering from chronic illness or during recovery from other conditions where anorexia is involved. Provision of such information to owners may also mean that anorexic cats can be successfully encouraged to eat at home, depending on the underlying condition, thus negating the stress associated with hospitalization.
Conclusion
From this investigation, it can be concluded that when attempting to encourage voluntary food intake in anorexic cats, perseverance is essential, irrespective of which feeding method is applied. The use of hand feeding or feeding smelly, moist, warmed food, were most successful in encouraging voluntary food intake in comparison to, feeding diet fed at home.