
It is estimated that 4–27% of all new-born puppies die in the first few weeks of life (Anderson, 1957; Bowden et al, 1963; Gill, 2001’ IndrebØ et al, 2007; TØnnessen et al, 2013; Scully et al, 2016). In the author's opinion these losses could be minimised by early intervention. Puppies should be weighed every 24 hours at the same time of day to identify those individuals failing to thrive. Certain circumstances dictate hand rearing the whole litter whereas, in other situations, only one puppy may require assistance.
Any puppy that is failing to thrive requires a full clinical examination, taking into consideration the ‘bigger picture’ to include the dam, her breeding history, the littermates and the environment. It may not always be clear what the problem is initially but the main point is to intervene quickly.
Hand feeding options
There are essentially two means of providing nutrition to newborn puppies: orogastric (‘stomach’) tube feeding and teat feeding (Harmar, 1974; Baines, 1981).
If a puppy lacks the suck reflex, then feeding by a tube placed into the oesophagus at each feed is the only option of providing nutrition via the gut. To test for a suck reflex, a clean finger is introduced into the puppy's mouth; a strong heathy puppy should latch on and suck the finger fairly strongly. Puppies often lack the suck reflex if they are premature, immature, hypothermic or hypoglycaemic.
Tube feeding is useful but should only be used when needed as there is a risk of placing the tube into the trachea rather than into the oesophagus. This risk increases as the puppy becomes stronger and more active. Tube feeding should only be necessary for a few days at most. Exceptions to this are puppies with abnormalities such as cleft palate and macroglossia. Tube feeding can be used to give oral rehydration solutions or milk substitute formula. Milk substitute formula is contraindicated in hypothermic and premature puppies (Williams, 1989; Bloomfield, 2013) as they are unable to digest milk or milk substitute. In these puppies electrolyte solutions are advised which provide hydration, electrolytes and some calories in the form of glucose without requiring digestion.
If the suck reflex is present then teat and syringe feeding is the method of choice. It is safer once the puppy is strong enough to suckle and most people find it easier than the traditional teat and bottle feeding. Feeding using a dropper bottle is not advised and often results in inhalation pneumonia (Bloomfield, 2013).
Orogastric tube feeding
Equipment:

Measuring the tube
The tube must be measured and marked before placing into the puppy. Every few days, as the puppy grows, the tube should be remeasured.
The end of the tube is placed at the level of the 9th rib (about ¾ along the length of the thorax, Figure 2). Then, with the puppy in a natural lateral position, the rest of the tube length should be laid along the lateral chest, up the neck and measured to the mouth. Fingers should be placed on the tube where the mouth and tube meet and a piece of surgical tape wrapped around the tube at this point. During feeding, the end of the tube should be sitting in the oesophagus just proximal to the stomach.

Placing the feeding tube
The feed should be warmed to body temperature (37oC) and the required volume drawn up into the syringe. Any air present in the syringe should be expelled. The syringe can then be connected to the feeding tube and the plunger pressed until a small drop of feed comes out of the end of the tube. This drop of feed can be used to lubricate the tube as it passes into the mouth and down into the oesophagus.
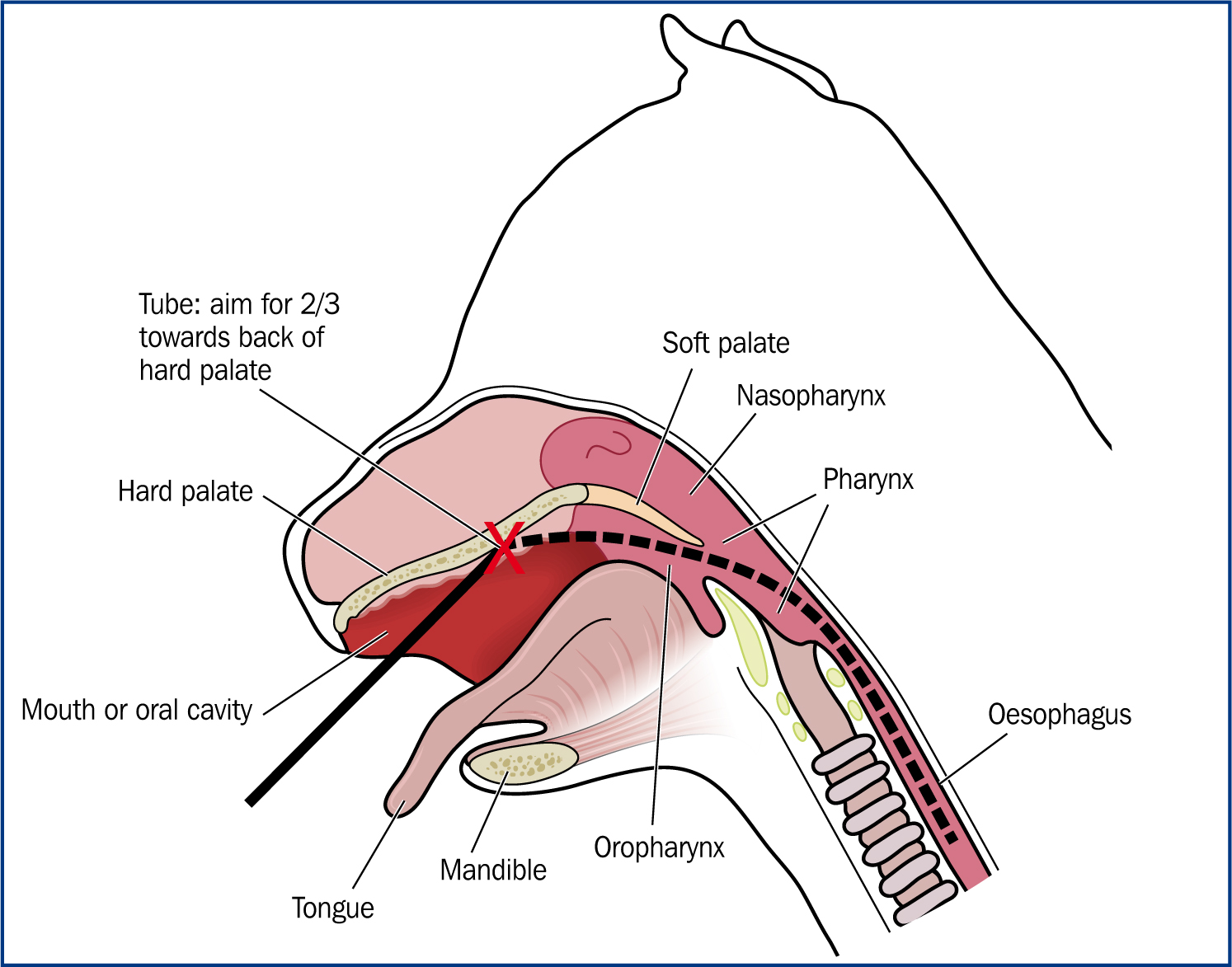
During feeding the puppy should be placed on a warm, non-slip surface. Using the thumb and forefinger of one hand, the corners of the mouth are gently pressed to make the puppy open its mouth; then, using the forefinger, gently ‘wedge’ the jaw open while the feeding tube is introduced with the other hand. Keeping the puppy's neck in a natural position, the tube tip is gently inserted into the mouth, aiming towards the hard palate, about ¾ of the way back. If the puppy's neck is extended or flexed, it is much harder to place the tube correctly into the oesophagus.
The tube should glide easily from the mouth and into the oesophagus (Figures 3 and 4). Once the surgical tape marker is at the puppy's lips the tube should be in the correct position.

Gliding the tube along the tongue will introduce the tube into the trachea. Attempting to place the tube with the neck flexed will also make tracheal entry more likely. The tube is in the trachea if it feels ‘sticky’ when advancing and if the tube cannot be advanced up to the tape marker. Puppies under 10 days of age and weak puppies requiring tube feeding usually do not have the cough reflex one would normally expect if the tube enters the trachea (Macintire, 1990).
Tube placement can be checked by pinching the puppy's ear; if strong enough, the puppy should be able to give a loud squeal. If it gags or chokes, the tube should be withdrawn. It is important to note that a weak or very young puppy may not react. Once the tube is placed correctly fingers are used to hold the tube in place during feeding (Figure 5). Failing to hold the tube in place will permit the tube to work its way back up the oesophagus during feeding and risk the feed entering the lungs. The syringe plunger is depressed slowly at a rate of one millilitre over 10 seconds. The tube should be left in situ for two seconds before removing in one smooth, swift movement.

If it has taken a few attempts to place the tube the feed in the syringe and the tube may need to be re-heated.
Teat and syringe feeding
Once a suck reflex is present, teat and syringe feeding is particularly useful for small and weak puppies as, by depressing the syringe plunger slowly, feeding is aided and the puppy does not need to expend so much energy obtaining its feed. Using a closed system in this way also helps avoid the puppy taking in air, which often happens when using a bottle. The best teats by far are ‘Catac’ feeding teats (Figure 6).

There are three different sizes of Catac teats. The ST1 (long and thin) is best for very small puppies and fits directly onto a syringe. The puppy only takes the tip of the teat into its mouth. The ST2 teat with a ridge suits most small to medium-breed puppies at birth; the puppy takes the teat up to the ridge into the mouth. The largest ST3 teat suits large and giant-breed puppies at birth in addition to smaller breeds moving on from the ST2 as they grow. Both the ST2 and the larger ST3 need an adapter to fit onto a syringe (Figure 7).

Adaptors
Adaptors can be fashioned from:
Teats
The teats are blind ending when purchased and so a hole needs to be made in the end. It can take some practice to make a hole small enough and there may be a few wasted teats in the beginning. For this reason it is always advisable to purchase more than is initially thought necessary.
A hole can be made using a small pair of fine, sharp scissors. The hole needs to be much smaller than would be used for bottle feeding. The hole size can be tested with a syringe of water; a small squirt of water needs to come out of the teat in a constant flow as the syringe plunger is depressed. It should not drip out of the teat.
When ready to feed the required warmed volume of feed can be drawn up in the syringe and the teat attached with an adapter if required. The end of the teat is dipped into some warmed feed to encourage the puppy to accept and latch onto the teat.
As with tube feeding, the puppy is placed on a warm, non-slip surface for feeding. Using the thumb and forefinger of one hand gentle pressure is applied to the corners of the mouth to make the puppy open its jaws. The forefinger is then used to wedge the mouth open while the teat is introduced into the mouth. The thumb and forefinger remain either side of the mouth to help the puppy stay on the teat if needed. The puppy should be held on the non-slip surface during the feed with the mouth, teat and syringe all kept in a level plane. The puppy should never be held on its back. As the puppy sucks from the teat, the puppy can be aided if necessary by slowly and smoothly depressing the syringe plunger (Figure 8). Pulling the teat gently away from the puppy can encourage the puppy to latch on. The puppy may take a little time to accept the teat, but will improve after a few feeds. Sometimes a change of teat size and shape helps acceptance. Older stronger puppies will ‘rear’ up onto their back legs to feed and may need to be gently held back from the teat.

Conclusion
Training and competency with the hand feeding techniques described in this article is a useful addition to a veterinary nurses's repertoire. Tube feeding can truly be a lifesaving technique and, once mastered, can be applied to many different species. It can seem daunting at first but is relatively straightforward providing the instructions given above are adhered to. Teat and syringe feeding is a natural follow on from tube feeding and helps weaker neonates get to grips with teat feeding.