

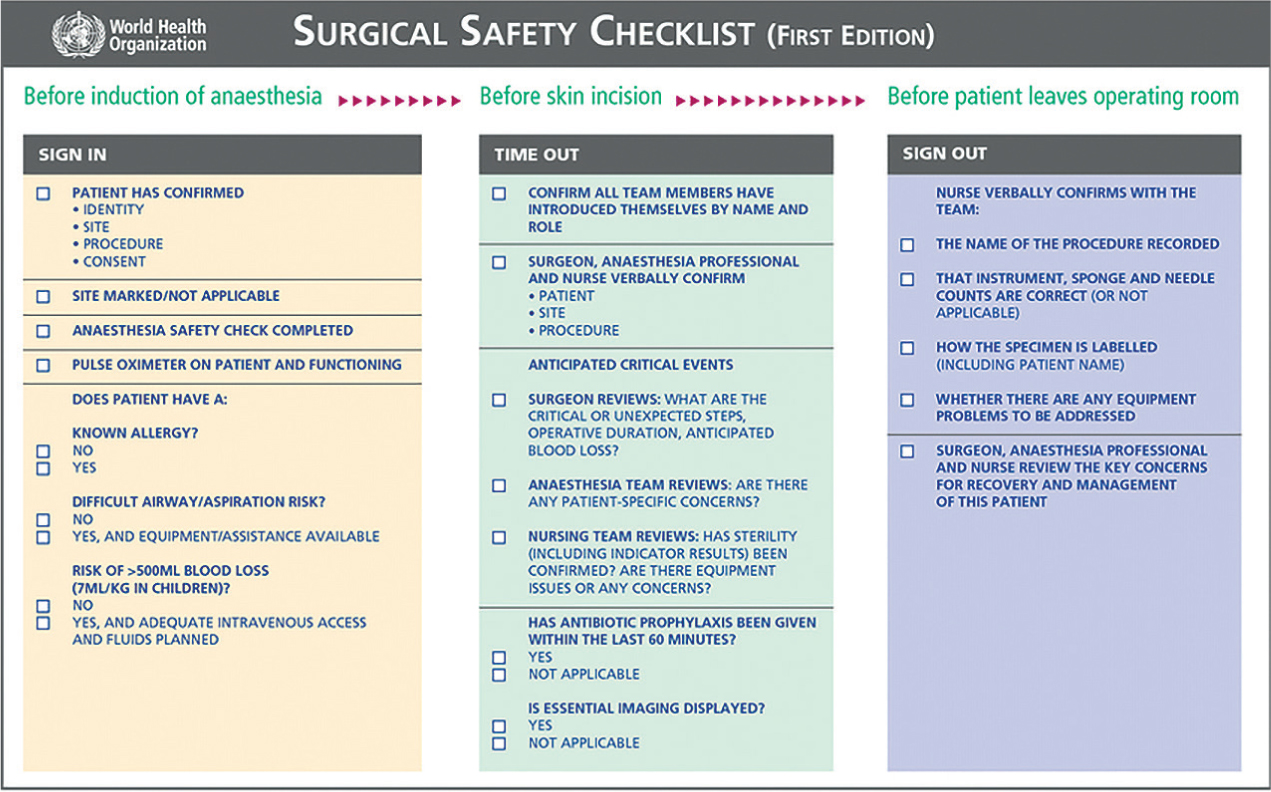
The introduction and development of the World Health Organization (WHO) surgical safety checklist in 2008 (Figure 1) led to considerable interest within the medical community regarding the proposed benefits of using a surgical safety checklist. An initial study identified a reduction in both inpatient complications and mortality with use of a surgical safety checklist (WHO, 2009a). After this study, the results led to repeated research (Van Klei et al, 2012), and soon surgical safety checklists were adopted throughout human healthcare as a way to reduce mortality and complication rates (Haynes et al, 2009; Conley et al, 2011). Surgical safety checklists are now used in all National Health Service hospitals throughout the UK (Bradbrook, 2018).
More recent authors have suggested that the benefit of using a surgical safety checklist may be directly linked to effective implementation, training and compliance of staff members. Subsequently, the importance of appropriate surgical safety checklist design, adaptation to the specific environment the surgical safety checklist is to be used in, and reduction of barriers to implementation has been highlighted (de Vries et al, 2010; Gasson and Wager, 2013; Menoud et al, 2018).
Why do I need a surgical safety checklist?
Human error is not predictable, many factors affect our ability to perform at our best. The full integration of the surgical safety checklist to the usual working practice of the hospital would ensure that critical steps were not missed, and potential problems were prepared for throughout the usual working day as well as into the area of out-of-hours care (Clapham, 2015). This will have a beneficial effect, therefore, on the instance of errors, patient safety and the associated self-deprecation of hospital staff when errors occur (Mosedale, 2020). Studies have reported significant improvement in surgical outcomes with a potential 47% reduction in deaths, 36% reduction in postoperative complications and 48% reduction in infections (Bergström et al, 2016; Haynes et al, 2017; Mehta et al, 2018). Feedback from teams using the WHO surgical safety checklist indicated that 78% believed the checklist had prevented an error (Haynes et al, 2009; Fudickar et al, 2012). There is also the instance within the veterinary profession of performing more complex and invasive surgery on patients with more intricate techniques filtering down through the medical profession. With these surgeries comes the increasing risk of postoperative complication (McMillan et al, 2014; Orjefelt, 2021).
The three-part checklist the WHO drafted in 2007 required that the usual course of anaesthesia and surgery be interrupted at three specific times, so that important information could be checked and communicated to all team members. These three times are immediately before the induction of anaesthesia (sign in), immediately before the skin incision (time out) (Figure 2), and right after skin closure (sign out). The first check would usually be carried out by the anaesthetist and consists of a check on the patient's identity, the procedure to be performed and other points relating to the anaesthesia. In the second check, the patient's identity and procedure is confirmed again, all team members are introduced, and all-important aspects of the operation itself are communicated. In the last check, important concluding points are checked such as sharp and swab count (Fudickar et al, 2012).

A good checklist
A good checklist should be:
- Concise
- Brief
- Actionable
- A verbal exercise between team members
- Modified for specific needs
- Tested before integration
- Integrated fully to usual working practice (Dugdale et al, 2020).
Dugdale et al (2020) made an interesting note that medical professionals consider themselves less fallible than aviation pilots do, and this sets them up for failure and the emotional psychological stress that goes with such failure. Veterinary professionals have similar attitudes towards infallibility, and the unrealistic outcome of this approach contributes to poor mental health and career dissatisfaction. Dugdale et al go on to say that recent safety culture has revealed significant overlap and commonality between veterinary and medical errors.
There are two systematic reviews of the WHO checklist that give a helpful summary of the evidence (Bergs et al, 2014; Treadwell et al, 2014).
Box 1.Points for inclusion in a surgical safety checklistSign in
- Patient and procedure identification
- Consent obtained
- Current medications checked
- Anaesthetic machines checked
- Anaesthesia risks identified (airway, allergies, co-morbidities)
Time out
- Patient and procedure identification
- Surgical risks identified (haemorrhage expected, procedure difficulties)
- Anaesthesia risks communicated to surgical team
- Patient prep complete (Figure 3) and sterility checks for instruments
- Swab count performed

Figure 3. Surgical final prep performed.
Sign out
- Instrument and swab count performed
- Sharps removed
- Specimens labelled
- Removal of throat packs/rectal plugs
- Recovery plan communicated (recovery risks, hospitalisation sheet written, medications prescribed, analgesic plan including rescue analgesia)
How do I get a surgical safety checklist for my practice?
The effective implementation of an adapted surgical safety checklist is an important but complex procedure (Menoud et al, 2018). Any practice wishing to implement a surgical safety checklist may find many barriers to overcome, including but not limited to, lack of leadership to implement, timing delays, training, forgetfulness or unfamiliarity of staff and lack of adequate staffing levels (Bergs et al, 2015; Willassen et al, 2018; Hawker et al, 2021).
There is importance placed on the adaptation of a ‘standard’ surgical safety checklist to any practice wishing to adopt one. Consider the list above detailing what a ‘good’ checklist should be. Think about what is pertinent to your practice. What kind of operations do you undertake most? Where have you encountered problems in the past?
There are basic points of the surgical safety checklist that should be included in any adaptation. Along with those this author would consider other points as well, which would lead to an example surgical safety checklist along the lines outlined in Box 1.
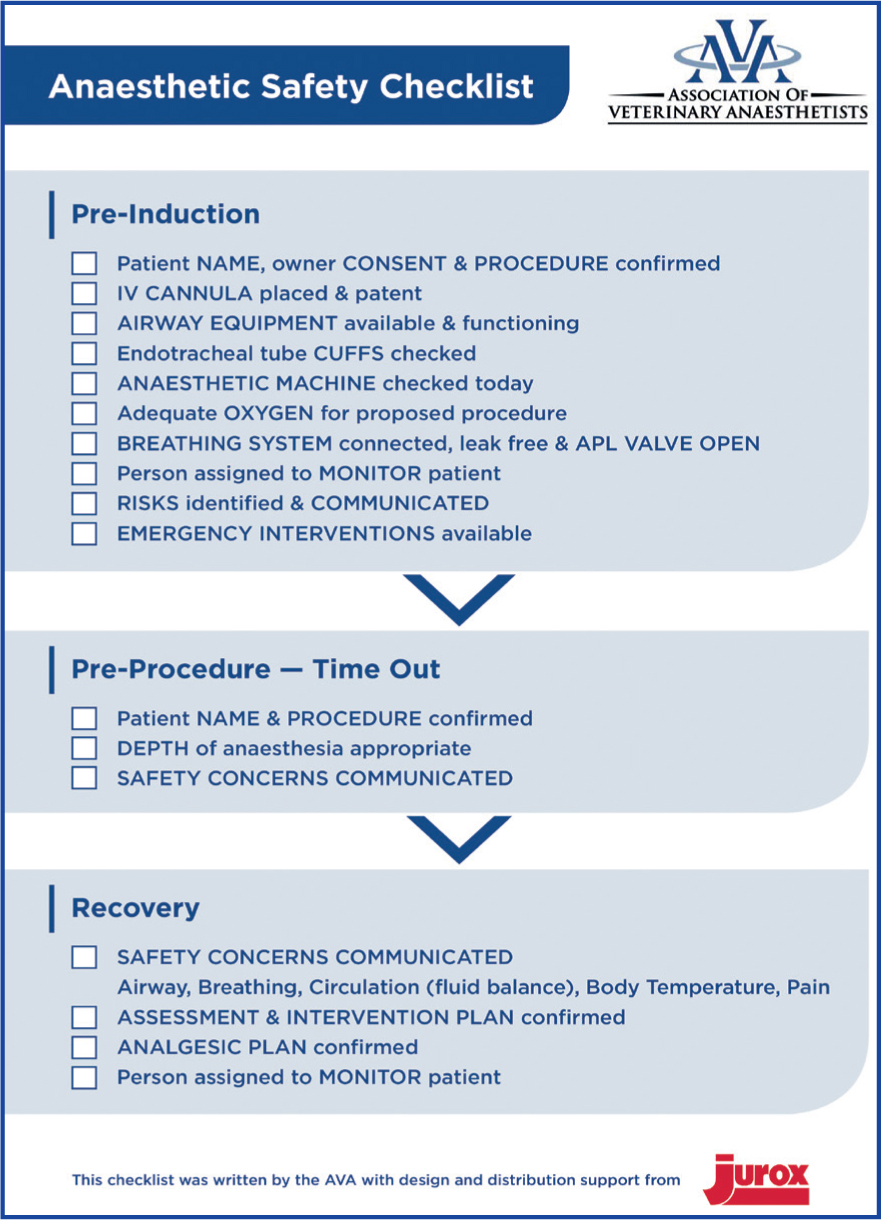
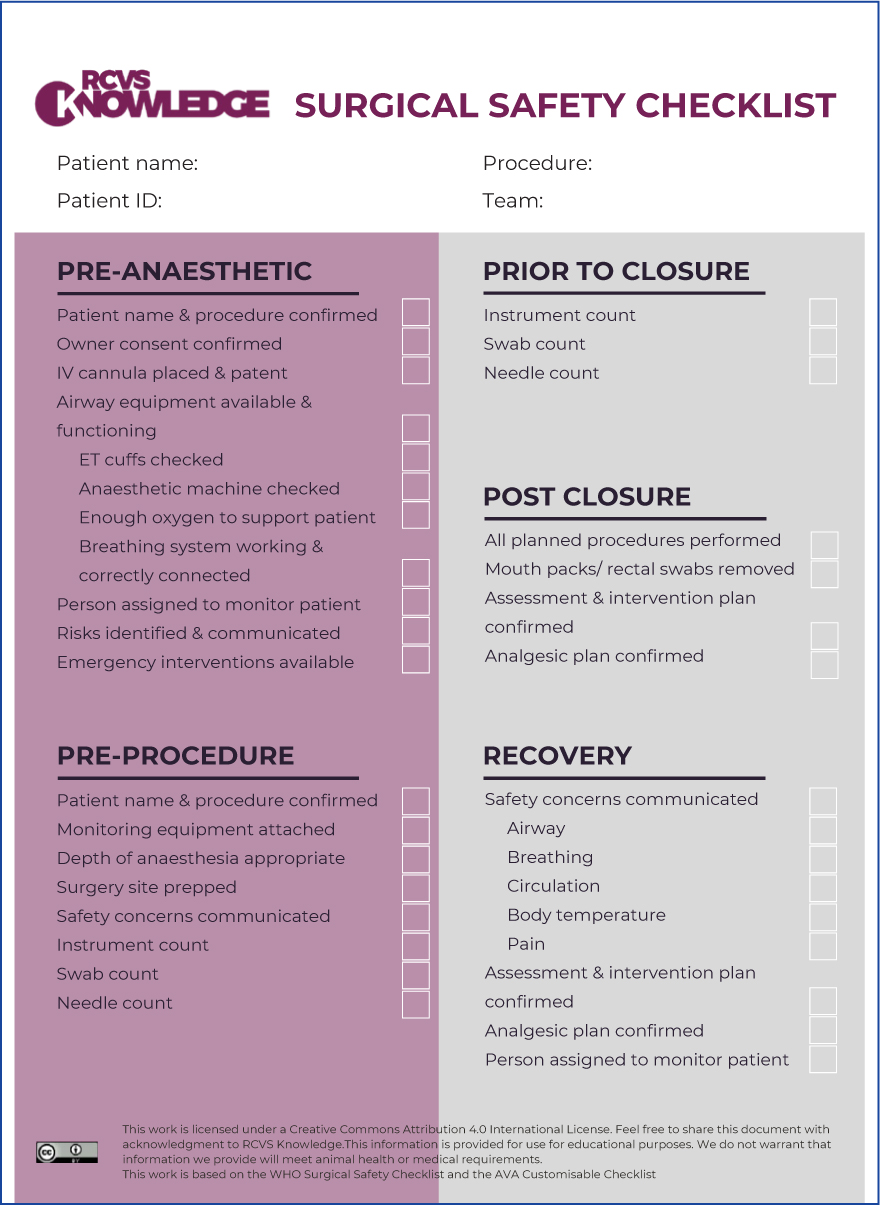
An example surgical safety checklist from the Association of Veterinary Anaesthetists (AVA) and Royal College of Veterinary Surgeons (RCVS) Knowledge can be seen in Figure 4 and 5. These are freely downloaded from the relevant websites.
In this author's experience the surgical safety checklist is usually a hard copy attached with the anaesthetic record. It is individual to each patient and can be included in the patient's care record. However, there are other ways to include a surgical safety checklist without being so individual. In some medical theatres the SSC is laminated on the wall in each theatre and a ‘checklist completed’ portion to the anaesthetic record has been added. It can, however, be argued that the sign in section is one of the most important, because completion will prevent anaesthesia of the incorrect patient and preparation for the incorrect procedure, as well as highlighting main causes for concern regarding patient status. Therefore, if this style is adopted, inclusion of this section may need to be added elsewhere.
It is important to note here that the surgical safety checklist is not simply a box ticking exercise, but a verbal challenge and response initiative between theatre team members. At each point on the surgical safety checklist the question should be verbalised with an informative answer as the response. If any answer is unknown, the procedure should be delayed or postponed until the appropriate information is obtained (Royal College of Veterinary Surgeons (RCVS) Knowledge, 2020).
I want a surgical safety checklist — what do I do next?
Research and investigate some of the different surgical safety checklists that are available to download, such as that produced by the Association of Veterinary Anaesthetists (AVA) (Figure 4) and RCVS Knowledge (Figure 5). Adaptation of the surgical safety checklist to each practice will be necessary so it is important to choose a current surgical safety checklist that has similarities to the points the practice wants to address. If it is not clear what those points may be, then performing an audit can be a useful tool to highlight which parts of the practice's protocols may need attention, and then choosing a suitable current surgical safety checklist will be easier. The goal of the surgical safety checklist is to help ensure that teams follow a few critical safety steps to minimise the most common risks and errors that can endanger lives and wellbeing of patients (WHO, 2009b).
Before the adaptation process is started, it is important to get a consensus from the practice team, and to designate a checklist coordinator. It is also important to gain agreement from the principal veterinary surgeon/practice manager and hold a general meeting to impart and discuss the reasons that a surgical safety checklist should be used, and what to include on the one that is to be implemented. Many of the checks included in most surgical safety checklists are considered routine, but there are always opportunities to improve consistency and even the most advanced hospitals rarely accomplish all checklist points for every patient (WHO, 2009a). The surgical safety checklist must be designed and circulated on a trial period. Ideally each section of the checklist should take no longer than a minute to complete. Once the checklist has been in place and used by everyone, a second meeting can be held to discuss the good, the bad and any proposed changes. Surgeons, anaesthetists and nurses should be involved in the adaptation process to actively seek input from those groups that will be using the surgical safety checklist. This will help to make appropriate changes to the surgical safety checklist, but will also encourage the feeling of inclusiveness and compliance that is important to gain lasting changes in practice protocol (WHO, 2009a; Braham et al, 2014; Kilbane et al, 2020). Last, a final draft of the surgical safety checklist can be put into use and a process audit conducted to ensure good uptake and correct completion is being achieved. Re-auditing further down the line will make sure that current evidence or requirements are being utilised, and measure ongoing use of the surgical safety checklist (RCVS Knowledge, 2020).
It will also be worthwhile to obtain further training for staff to ensure that theatre users build an appreciation of how and why the surgical safety checklist works to gain knowledge of how safer care is achieved. Each section of the surgical safety checklist has merit with regard to patient safety and so each should be addressed properly (Conley et al, 2011).
I've designed a surgical safety checklist — how do I implement it?
Begin by working with those clinicians who are interested in implementing the surgical safety checklist into their anaesthetic and operating regimen. Start small by testing out the checklist in one operating theatre with one team, and moving on to include others after momentum grows and initial problems have been addressed. In order to use the checklist a single person must be made responsible to challenge each section and this is often the circulating nurse, but it can be any clinician participating in the procedure (WHO, 2009a).
All steps within the surgical safety checklist sections should be checked verbally with the appropriate team member to ensure that the important points have been actioned. For example, before induction the checklist co-ordinator will confirm out loud with the anaesthetist that the patient identity, the procedure, and the consent for that procedure are all confirmed. Before skin incision, the surgical team will confirm out loud the patient identity, the procedure, and their surgical concerns. Before leaving theatre, the surgical team will confirm out loud the swab and instrument counts, sharp removal, specimens obtained and discuss ongoing plans for the patient's postoperative management. Having that single person dedicated to the challenge and response of each section of the surgical safety checklist can ensure that no steps are missed in any rush to move on with the next phase of the procedure.
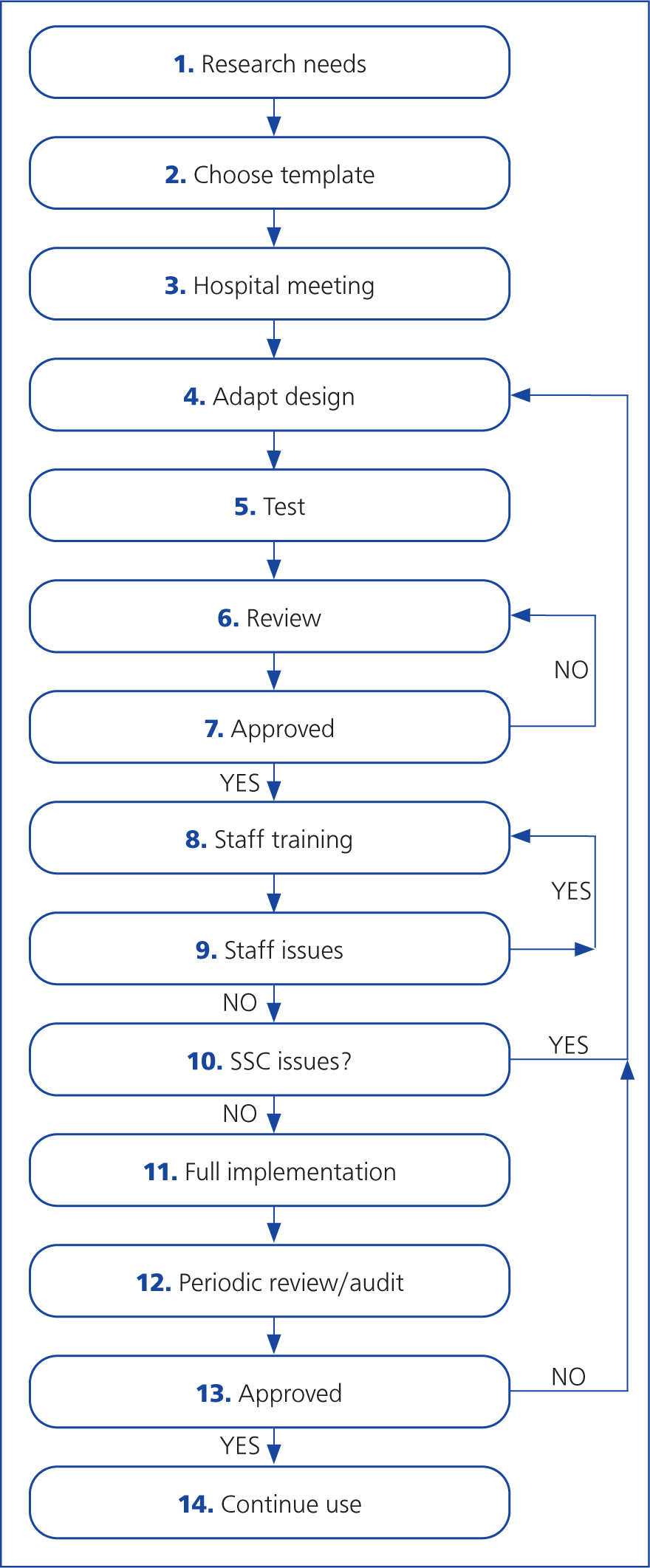
The flowchart in Figure 6 can be used as a guide to the design and implementation process.
Guide to flow chart for implementation
- Research where within your practice protocols for surgical patients the surgical safety checklist needs to focus.
- Choose an existing surgical safety checklist to be the template for the practice. The most ideal will be one that encompasses some of the points raised in step 1.
- Propose a hospital meeting to outline why it is necessary to implement a surgical safety checklist, give an evidence base to prove how the surgical safety checklist improves patient safety etc. This is where like-minded staff members will be identified, and where senior approval will be gained along with development ideas.
- Adapt the template surgical safety checklist chosen to encompass all the points required by the practice, and those raised in the hospital meeting. Make sure the surgical safety checklist is succinct and not over complicated.
- Test the adapted surgical safety checklist in a small setting with one surgical team within one theatre over a short period of time. Choose a team with enthusiastic staff members that are behind the surgical safety checklist implementation.
- Review the surgical safety checklist after the test, gaining feedback from those who have used it. This is when the surgical safety checklist can be adjusted if the test finds areas that need improvement or omission.
- Gain approval from practice staff and managers that the designed surgical safety checklist is appropriate.
- Hold a staff training session. This is where those staff members who will be involved in the use of the surgical safety checklist need to be trained in its proper use, and understand their role within the surgical safety checklist. Remember to designate a checklist coordinator in each team who will lead the verbal challenge and response.
- If there are staff members who are resistant to the idea of the surgical safety checklist or have unanswered questions, then further training can be sought.
- If the training session throws up issues with the adapted surgical safety checklist, then the design can be modified and you return to step 4 of this flowchart.
- If everyone is happy then continue with a full implementation of the adapted surgical safety checklist across the hospital as a whole.
- Periodically it will be prudent to review and complete a process audit on the compliance, completion of and improvement the surgical safety checklist has made. Ask: is the surgical safety checklist being used properly and filled in real-time and not retrospectively? Is the surgical safety checklist being used as a verbal or written exercise? Are the points raised in step 1 of the flowchart being addressed by the surgical safety checklist?
- If any changes need to be made to the surgical safety checklist after the audit, then the design can be modified, and you return to step 4 of this flowchart.
- If the surgical safety checklist is approved and no changes need to be made, then continue with its use.
Conclusion
It must be recognised by any practice wishing to implement a surgical safety checklist that doing so will take time for successful integration with current protocols. Completion of the surgical safety checklist should take no more than a few minutes each time and studies have shown no reduction in operating room efficiency when the surgical safety check-list is in use (Papaconstantinou et al, 2013). In order to ensure the surgical safety checklist does not impact on timings of the surgical day the WHO surgical safety checklist was not intended to be comprehensive, and so individual practices may consider having other safety checks in place for specific procedures not included in the adapted surgical safety checklist, and checklist co-ordinators are cautioned against making the surgical safety checklist needlessly complex (WHO, 2009a). With the availability of free-to-download veterinary surgical safety checklists the use of a surgical safety checklist is within the reach of any practice wishing to integrate it into daily routine. The improvement to patient safety with the use of surgical safety checklists cannot be denied and so further uptake to the veterinary profession can ultimately only be a good thing.
KEY POINTS
- Surgical safety checklists are within the grasp of any veterinary practice that wishes to implement one.
- Adaptation of a surgical safety checklist will be necessary to complement the practice into which it is to be integrated.
- Compliance of staff to the implementation of a surgical safety checklist is paramount to success.
- Full implementation of a surgical safety checklist will take time to achieve.