Boveri S, Brearley J All in a tangle: a mishap with an oesophagostomy tube in an intubated cat. Vet Anaesth Analg. 2015; 42:(2)227-9
Campbell JA, Jutkowitz A, Santoro KA, Hauptman JG, Holahan ML, Brown AJ Continuous versus intermittent delivery of nutrition via nasoenteric feeding tubes in hospitalised canine and feline patients: 91 patients (2002 – 2007). J Vet Emerg Crit Care. 2010; 20:(2)232-6
Chan DL Refeeding syndrome in small animals. In: Chan DL (ed). Chichester: John Wiley & Sons Ltd; 2015
Eirmann L Esophagostomy feeding tubes in dogs and cats. In: Chan DL (ed). Chichester: John Wiley & Sons Ltd; 2015
Firth A Early enteral nutrition – principles and practice. The Veterinary Nurse. 2013; 4:(7)392-9
Freeman L, Becvarova I, Cave N WSAVA Nutritional Assessment Guidelines. J Small Anim Pract. 2011; 52:(7)385-96
Gajanayake I Management of the anorexic cat. In Practice. 2014; 36:163-71
Gajanayake I, Chan DL Gastrostomy feeding tubes in dogs and cats. In: Chan DL (ed). Chichester: John Wiley & Sons Ltd; 2015
Han E Eosophageal and Gastric Feeding Tubes in ICU Patients. Clin Tech Small Anim Pract. 2004; 19:(1)22-31
Ireland LM, Hohenhaus AE, Broussard JD, Weissman BL A comparison of owner management and complications in 67 cats with esophagostomy and percutaneous endoscopic gastrostomy feeding tubes. J Am An Hosp Assoc. 2003; 39:241-6
Kealy RD, Lawler DF, Ballam JM Effects of diet restriction on life span and age-related changes in dogs. J Am Vet Med Assoc. 2002; 220:(9)1315-20
Lewis SJ, Egger M, Sylvester PA, Thomas S Early enteral feeding versus “nil by mouth” after gastrointestinal surgery: systematic review and meta-analysis of controlled trials. Br Med J. 2001; 323:1-5
Liu DT, Brown DC, Silverstein DC Early nutritional support is associated with decreased length of hospitalization in dogs with septic peritonitis: A retrospective study of 45 cases (2000–2009). J Vet Emerg Crit Care. 2012; 22:(4)453-459
Mansfield CS, James FE, Steiner JM, Suchodolski JS, Robertson ID, Hosgood G A pilot study to assess tolerability of early enteral nutrition via esophagostomy tube feeding in dogs with severe acute pancreatitis. J Vet Intern Med. 2011; 25:(3)419-25
Marks SL Nasoesophageal, Esophagostomy, Gastrostomy, and Jejunal Tube Placement Technique, 7th edn. In: Ettinger SJ, Feldman EC (eds). Philadelphia USA: Elsevier Health Sciences; 2009
Michel KE Preventing and Managing Complications of Enteral Nutritional Support. Clin Tech Small Anim Pract. 2004; 19:(1)49-53
Mohr AJ, Leisewitz AL, Jacobson LS, Steiner JM, Ruaux CG, Williams DA Effect of Early Enteral Nutrition on Intestinal Permeability, Intestinal Protein Loss, and Outcome in Dogs with Severe Parvoviral Enteritis. J Vet Intern Med. 2003; 17:791-798
Nutrition is one of the most important considerations in the maintenance of health and early intervention can play a critical role in ensuring successful patient outcome and management of disease. In veterinary patients, this is reflected by the recognition of nutritional assessment as the 5th vital sign. It is the responsibility of veterinarians and the veterinary nursing team to ensure the early identification of patients in need of nutritional support. Once nutritional intervention is deemed necessary, collaboration is essential to determine the most appropriate method and route of delivery, alongside the patient's nutrient needs and feeding goals. This article outlines a practical, systematic approach to the placement of feeding tubes, a form of nutritional lifeline, frequently utilised in small animal practice.
There are numerous factors involved in the regulation of appetite. In hospitalised veterinary patients, those relating to underlying disease, procedure-induced stress, adverse effects of medications and hospital environment can result in a reduced desire to eat, warranting nutritional intervention (Gajanayake, 2014). The benefits of rapid initiation of feeding are highlighted in current literature, across both the veterinary and human fields of medicine, with enteral feeding methods considered preferable to parenteral nutrition (Lewis et al, 2001; Campbell et al, 2010; Mansfield et al, 2011). A feeding method that utilises as much of the functioning gastrointestinal tract as possible should be adopted, while also ensuring its suitability for the patient's condition and initial hospitalisation period (Gajanayake, 2014).
This article outlines a step-by-step approach to the placement of feeding tubes, frequently utilised in small animal practice. Readers should be aware that published variations to these methods do exist and the methodology used in veterinary practice will be subject to the personal preference of the veterinarian (VS) overseeing the patient's care and treatment. An overview of the advantages and disadvantages of each tube is provided in Table 1. Depending on the geographic location in which veterinary nurses (VNs), or technicians, are practising, the legal right to place a feeding tube will be dictated by the relevant regulatory body in that area. While the placement of certain feeding tubes is reserved only for veterinarians, an understanding by VNs and technicians of the technique used is essential to the delivery of optimal patient care. In the UK, under The Veterinary Surgeons Act 1966 (Schedule 3 Amendment) Order 2002, Registered VNs are permitted to place naso-oesophageal (NO) and naso-gastric (NG) feeding tubes. Student VNs undertaking the small animal pathway of training, and working at the direction of their VS employer, are required to undertake assisted feeding, including managing and maintaining feeding tubes under supervision.
Naso-oesophageal and naso-gastric
Oesophagostomy
Gastrostomy
Advantages
Disadvantages
Advantages
Disadvantages
Advantages
Disadvantages
Non invasive
Generally well-tolerated
Does not prevent animal from eating and drinking
Suitable for patients that are considered too unstable to undergo sedation or general anaesthesia
Easy to place with minimal chemical restraint and topical local anaesthesia
With training, these tubes can be managed by owners at home
Not suitable for patients that are vomiting, unconscious, have a poor gag-reflex or megaoesophagus
Easily dislodged so a buster collar required
Limited by the small bore of the tube and hence the type of diet used
Only suitable for use in the short term (i.e. up to 5 to 10 days)
May be vomited up
Complications include rhinitis, epistaxis, tracheal intubation
Simpler to place than gastrostomy tubes
Large bore tubes can be used
Generally, well tolerated (especially by cats)
Indicated for patients requiring longer-term nutritional support and/or bypass of the oral cavity or oropharynx
Animals are able to eat via the oral route in spite of the tube
Generally used for short to mid-term nutritional intervention but can be used for prolonged periods
Liquid diets or blenderized tinned diets can be used
Feeding can begin immediately after placement, once patients have recovered fully from anaesthesia and can be removed at any time
With training, these tubes can be managed by owners at home
Requires general anaesthesia for placement
Placement involves a surgical procedure
Stoma site can become infected
Complications include inadvertent placement in the trachea or mediastinum, damage to major blood vessels or nerves, stomal inflammation and infection
Cannot be used for patients with persistent vomiting, altered mentation and oesophageal disorders
Can be challenging to place in giant breeds and obese patients
Suitable for mid to longterm nutritional support
Wide diameter tube allows the use of a wider selection of feeds
PEG tubes can be bought as a complete kit or can be modified from a gastrostomy tube
In cases of prolonged use, PEG tubes can be modified to a low-profile feeding tube
With training, these tubes can be managed by owners at home
Not suitable for animals with persistent vomiting, gastrointestinal obstruction, altered consciousness, compromised wound healing/immunity or a compromised gastric wall
Placement requires general anaesthesia and laparotomy or specialised endoscopic equipment
Feeding is generally delayed until 12–24 hours following placement
Risk of severe complications such as peritonitis, if the tube becomes dislodged
Should remain in place for 7–10 days (or longer in hypoproteinaemic or immune-compromised patients) to allow adequate adhesions to form between stomach and abdominal wall
NO and NG tubes
NO and NG tubes provide short-term enteral nutritional support, generally for up to 5 to 10 days, and are suitable for use in patients for whom sedation or general anaesthesia is contraindicated (Aicher and Tobias, 2013). In addition to feeding, NG tubes can also be useful for aspirating residual gastric fluid in conditions such as ileus. The type of diet used is limited by the narrow bore of the tube, typically 3.5–6 Fr in cats and 8–10 Fr in dogs, to low viscosity and nutritionally complete liquid diet formulations. Examples include Royal Canin liquid diets, Formula V® EnteralCare™ KC (PetAg), CliniCare® (Zoetis) and Rebound® liquid diet (Virbac Animal Health).
Despite the selection of an appropriate diet, blockages remain a potential risk and can be minimised through careful flushing before, and after, feeding and by avoiding the administration of oral medications via NO and NG tubes. These feeding tubes are contraindicated in patients that are laterally recumbent or dyspnoeic and for those with altered consciousness, facial trauma, oesophageal dysfunction/obstruction or an inability to protect their airway. Use in patients with raised intraocular and intracranial pressure should also be avoided due to the risk of sneezing during placement. Potential complications of placement also include epistaxis, therefore care should be taken in patients with thrombocytopenia or coagulopathies.
Placement of NO and NG tubes
Ensure that the patient is restrained securely. The head should be held in a normal functional position, avoiding hyperextension or hyperflexion (Figure 1). The VS should decide if sedation of the patient is required and make the necessary arrangements for this to be done.
Tilt the patient's head upwards and place 4–5 drops of lidocaine, or proparacaine, hydrochloride solution into the nostril(s) (Figure 2). Application into both nostrils enables either to be used as required. Allow several minutes to take effect. The local anaesthetic may have a bitter taste, resulting in hypersalivation by the patient. Some practitioners also recommend adding a drop of proxymethacaine or lidocaine to the eye to aid in numbing the nasal passages.
If placing a NO tube, the distance from the nose to the seventh or eighth intercostal space should be measured. If placing a NG tube, the nose to the last rib should be measured. This position should be marked on the tube with a permanent marker pen or a small piece of tape.
To aid insertion, the tube can be lubricated with a water-soluble, or lidocaine, gel.
With the patient in a standing, sitting or sternally recumbent, position, one hand will steady the patient's head in a neutral position while the other inserts the tube. Cats: the tube should be inserted in the medial aspect of the nares and directed in a caudoventral direction. Dogs: the tube should be directed ventromedially and into the ventral meatus of the nasal cavity. Applying gentle pressure in between the nares can facilitate opening and elevate the proximal end of the tube, aiding insertion (Figure 3). A confident motion can prevent stimulation of sneezing.
The tube is passed until it reaches the predetermined position (nose to intercostal space). If resistance is felt, the tube should be withdrawn and redirected in a ventral direction.
To prevent unintentional removal, or displacement, the tube should be secured before verifying its position. One of the common methods used to confirm correct placement is to instill sterile saline down the feeding tube and observe for signs of coughing. The volume must be adapted for the size of patient but is usually between 1 and 5 mls. There should be no gurgling when auscultating the chest. More accurate methods involve either:
Connecting the feeding tube to a portable capnograph. A lack of visible waveform and an end-tidal carbon dioxide measurement of 0 mmHg will verify correct tube placement.
Taking survey or contrast radiographs of the thorax
pH assessment of fluid aspirated from the tube (Figure 4)
Aspiration with a syringe to check for a vacuum.
Securing of the tube can be achieved using square knot or finger trap sutures (with or without tissue glue) or skin staples, at a point level with the forehead or buccal pouch on the lateral face (Figure 5). The application of EMLA cream to the patient's nose or forehead prior to placing, and securing, the tube can increase patient comfort and compliance.
Figure 1. The patient must be restrained securely with the head held in a normal functional position.Figure 2. Local anaesthetic drops can be placed into the nostrils.Figure 3. Applying gentle pressure in between the nares can facilitate insertion of the tube.Figure 4. Correct placement of a naso-gastric tube can be confirmed through pH assessment of aspirated fluid.Figure 5. A naso-gastric tube secured using finger trap sutures.
To prevent patient interference and premature removal of the tube, a buster collar should be fitted. Once the tube is no longer required, it can be easily removed by cutting the suture material, or removing the staples, and pulling the tube out.
Oesophagostomy tubes
For patients requiring longer-term nutritional support and/or bypass of the oral cavity or oropharynx, oesophagostomy tubes are well tolerated and can be managed by owners at home. The larger bore (14–20 Fr) allows the feeding of a broader selection, and volume, of food, including blenderized diets. Despite these advantages, limitations include surgical placement, warranting general anaesthesia. Endotracheal intubation of the patient is desirable however, as reported by Boveri and Brearley (2015), care must be taken by the VS to avoid entrapment during placement of the feeding tube. Further, serious, complications include inadvertent placement in the trachea, or mediastinum, and damage to major vessels or nerves, therefore surgical competence should be assured prior to placement, together with careful verification of correct positioning afterwards.
Oesophagostomy feeding tubes are contraindicated in patients with persistent vomiting, altered consciousness and for those with oesophageal disorders or who have undergone oesophageal surgery. They can also be challenging to place in giant breeds or obese patients (Hodshon and Tobias, 2014). Feeding can begin immediately following placement (Eirmann, 2015), but should be instigated in consultation with the VS. To reduce the risk of aspiration pneumonia, patients should have recovered fully from anaesthesia and be able to support themselves in a sternal position.
Placement of oesophagostomy tubes
Proper placement of an oesophagostomy feeding tube requires the distal tip to be placed in the mid cervical oesophagus to the level of the fifth to ninth intercostal space. This may require premeasuring of the tube.
ather than cutting the distal tip and creating a sharp edge, the exit side hole should be elongated using a small blade. This will help prevent clogging of food.
The patient should be anaesthetised and preferably intubated. While in right lateral recumbence, the left side of the neck should be clipped and aseptically prepared using a routine surgical scrub (Figures 6 and 7).
With the tips facing outwards, a curved Rochester-Carmalt forcep (or a curved haemostat) is placed into the mouth and down the oesophagus to the mid-cervical region (Figure 8). The jugular vein should be identified and avoided.
The tip of the Carmalt is pushed dorsal to the jugular vein, pressing the oesophagus towards the skin.
The tip of the Carmalt is palpated over the skin to confirm its location (Figure 9). Avoiding any nearby neurovascular structures, a stab incision is made through the skin and into the oesophagus. The mucosa of the oesophagus is relatively more difficult to incise than the skin.
The tip of the instrument is pushed through the incision, which can be slightly enlarged with the blade.
The Carmalt is opened slightly and tip of the oesophagostomy tube is placed within the jaws of the instrument (Figure 10).
The Carmalt is then clamped closed and pulled from the oral cavity (Figure 11).
The tips of the Carmalt are disengaged and the tip of the tube is curled back into the mouth and fed into the oesophagus (Figure 12). As the curled tube is pushed into the oesophagus, the proximal end is gently pulled simultaneously.
This will result in a subtle ‘flip’ as the tube is redirected within the oesophagus. The tube should easily slide back and forth a few millimeters, confirming that the tube has straightened within the larynx (Figure 13).
A visual inspection will confirm that the tube is no longer present within the oropharynx.
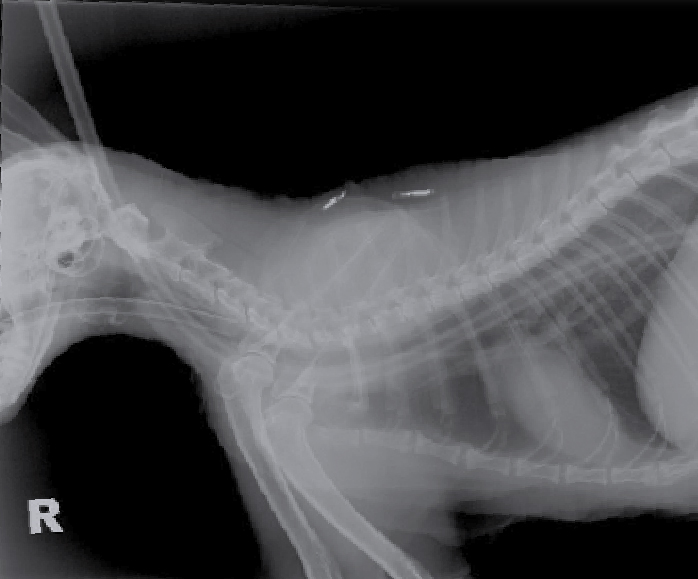
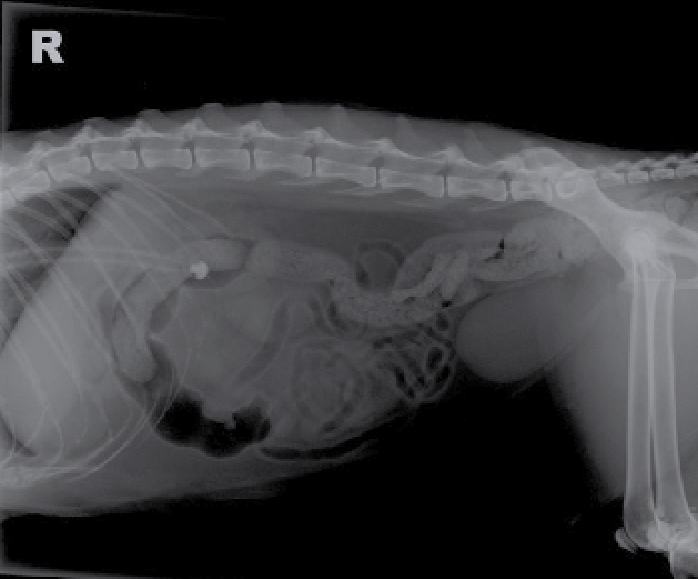
A thoracic radiograph will confirm correct placement of the tube in the mid to distal oesophagus (Figure 14). The tip of the tube should not pass beyond the lower oesophageal sphincter (Figures 15 and 16) as this can cause irritation and predispose the patient to gastric reflux (Hodshon and Tobias, 2014).
The tube is secured using a Chinese finger trap, or Roman sandal, suture pattern (Figure 17). The use of a purse-string suture around the stoma is documented, but associated with cellulitis and peristomal inflammation (Hodshon and Tobias, 2014).
The incision site can be gently cleaned before placing a light bandage (Figure 18). Despite a limited supporting evidence base, some authors, including Eirmann (2015), suggest the application of antibiotic ointment to the stoma site.
Figure 6. Initial aseptic preparation of the neck using diluted chlorhexidine.Figure 7. Final aseptic preparation of the neck using ChloraPrep 2% with Tint in a 3 ml applicator.Figure 8. A curved Rochester-Carmalt forcep is placed into the mouth and down the oesophagus to the mid-cervical region.Figure 9. The tip of the Carmalt is palpated over the skin before making a stab incision.Figure 10. The tip of the oesophagostomy tube is placed within the jaws of the instrument.Figure 11. The Carmalt is clamped closed and pulled from the oral cavity.Figure 12. The tip of the tube is curled back into the mouth and fed into the oesophagus.Figure 13. The tube in situ within the oesophagus.Figure 14. A radiograph demonstrating the correct placement of an oesophagostomy tube in the mid to distal oesophagus of a cat.Figure 15. A thoracic radiograph of a cat, illustrating the incorrect placement of an oesophagostomy tube. Note the tip cannot be seen on this view.Figure 16. Note the tip of the oesophagostomy tube situated, incorrectly, beyond the gastroesophageal junction in a cat.Figure 17. Chinese finger trap suture to secure an oesophagostomy tube.Figure 18. A light bandage to secure and protect the tube.
While complications associated with O-tubes are generally minor (Hodshon and Tobias, 2014), these may include tube obstruction, stomal infection and abscessation, peristomal dermatitis or cellulitis and inflammation (Ireland et al, 2003). Swelling of the head and neck can also result due to an excessively tight bandage. While rare, vomiting can lead to dislodgement of the tube, resulting in a foreign body. Once oral food intake is sufficient to meet the patient's caloric requirement, the tube can be removed. This can easily be performed by cutting the suture material and pulling the tube, leaving the wound to heal via second intention.
Gastrostomy tubes
Gastrostomy feeding tubes offer the provision of mid to long-term nutritional support via entry into the stomach; adequate gastrointestinal function is therefore essential (Marks, 2009). The wide diameter tube, often 15 Fr for cats and 19–24 Fr for medium to large dogs, enables easy administration of food from a wider selection of diets in comparison to smaller diameter tubes. Placement requires general anaesthesia and either laparotomy or percutaneous approach, the latter involving a blind or endoscopic technique using specialised equipment. Feeding is generally delayed for at least 12–24 hours with either method (Snyder, 2009) and endoscopic placement can affect gastric motility for up to 3 days (Gajanayake and Chan, 2015). Tubes usually remain in place for a minimum of 7 to 10 days, often longer in hypoproteinaemic or immune-compromised patients. This allows adequate adhesions to form between the stomach and abdominal wall, preventing leakage of stomach contents and subsequent peritonitis (Snyder, 2009).
The use of gastrostomy tubes is contraindicated in patients with persistent vomiting, gastrointestinal obstruction, compromised gastric wall and altered consciousness (Marks, 2009). Endoscopic placement in larger breeds of dog (weighing 30 kg or over) is also contraindicated due to tendency for migration of the feeding tube and subsequent peritonitis (Snyder, 2009). Incorrect placement can cause abdominal visceral injury and pyloric outflow obstruction. Further complications include dehiscence, cellulitis and infection of the stoma site. Overly tight securing of the tube can also result in pressure necrosis. Careful patient evaluation and selection, appropriate selection of feeding tube, correct surgical technique and competence, accurate patient monitoring and adherence to the prescribed feeding regimen can limit potential complications (Gajanayake and Chan, 2015).
Placement of gastrostomy tubes
The following methodology describes the placement of a percutaneous endoscopically placed gastrostomy (PEG) tube using a commercial kit.
The patient should be placed in right lateral recumbence, enabling entry of the tube through the greater curvature of the stomach and left body wall.
Clip and surgically prepare the skin over the lateral abdominal wall and caudal to the left costal arch.
A mouth gag is placed between the right upper and lower canine teeth before the endoscope is passed down into the stomach.
Following slight inflation and distension of the abdomen, the position for insertion of the PEG tube is located on the anterior abdominal wall by either:
Transabdominal impulse — endoscopically visible bulging when the surgical assistant presses the wall (Figure 19) or
Trans-illumination after dimming the light in the room.
Under direct endoscopic view, a small stab incision is made into the stomach, adjacent to the endoscope tip and a 16–18 G, 1.5–2 inch, catheter punctures the body wall and into the stomach (Figure 20).
The needle is removed, leaving the cannula in place.
The placement wire (introduction line) is advanced through the cannula and the loop is grasped with endoscopic retrieval forceps (Figure 21).
The wire is then pulled out through the mouth as the endoscope is withdrawn.
The placement wire is looped through the PEG tube.
Gentle traction is applied to the placement wire through the puncture cannula, while guiding the PEG tube through the mouth (Figure 22).
When the tip of the PEG tube reaches the puncture cannula, some resistance will be felt. The puncture cannula is removed and the conical end of the PEG tube is gently pulled through the incision. It may be necessary for the VS to extend the incision slightly using a scalpel blade.
The PEG tube is pulled through the abdominal wall until the inner retention plate (mushroom tip) touches the inner gastric wall (Figure 23).
The guiding thread of the PEG tube is cut close to the cone. A plastic fixation plate and clamp is placed over the tube before it is capped (Figure 24). In cases of prolonged use, PEG tubes can be modified to be low-profile.
A light bandage, or stockinette, can be fitted to protect the tube. A non-adhesive dressing, with or without antibiotic ointment, can be used to cover the stoma site.
Figure 19. Locating the position for insertion of the PEG tube.Figure 20. A stab incision being made by a veterinarian into the stomach.Figure 21. A placement wire being advanced through the cannula.Figure 22. The PEG tube being guided out through the mouth.Figure 23. The PEG tube being pulled through the abdominal wall.Figure 24. Placement of the plastic fixation plate (nearest to the body) and clamp (situated further up) over the tube.
Once oral food intake is sufficient to meet the patient's caloric requirement, the tube can be removed. In medium to large dogs, the PEG tube can be cut close to the body wall and the mushroom tip pushed into the stomach and passed via faeces. For cats and small dogs, this method could result in intestinal obstruction and thus, the tube can be removed using quick traction via the stoma site or via anaesthesia and endoscopic retrieval via the mouth (Han, 2004). The gastrointestinal tract should seal with minimal or no leakage within 24 hours.
Feeding tube management and prevention of complications
The following points should be considered in the use of all enteral feeding tubes:
Before implementation of any nutritional plan, the patient must be cardiovascularly stable and have major electrolyte, fluid, and acid–base abnormalities corrected (Freeman et al, 2011). Provision of supportive care that addresses problems involving hydration and electrolyte status, pain, body temperature, vitamin B deficiencies and nausea can result in appetite being re-established in many anorexic patients (Gajanayake, 2014).
To avoid inadvertent delivery of an inappropriate substance into a feeding tube, or food into an intravenous catheter, both must be clearly labelled. The use of enteral feeding safety devices, including colour coded enteral syringes, tubing and adapters, are also recommended.
The selection of the widest possible feeding tube will ease the delivery of food and prevent blockages. Tubes should be flushed with warm water before feeding to confirm placement and again afterwards to ensure patency of the tube and delivery of the full volume of food. Flush volumes must be taken into consideration when determining appropriate meal sizes. The patient and tube size will dictate the amount of water required. Generally, a small volume (around 5 ml) is delivered prior to feeding and between 10 ml (for liquid diets) and 20 ml (for blenderized diets) after feeding (Hodshon and Tobias, 2014).
A buster collar should be fitted to prevent iatrogenic tube removal.
It is important to allow patients a chance to feed naturally, before delivery of each tube feed. This will allow for monitoring of the return of normal appetite and improvement in condition.
Aspiration pneumonia is a potentially fatal complication of enteral tube feeding. Risk factors include absence of a gag or cough reflex, laryngeal disease, impaired mental status and neurologic injury. Working with the VS to ensure selection of the most appropriate feeding tube and feeding practice, together with careful patient monitoring, will help to minimise risk. Patients should be fully conscious and, where possible, positioned in sternal recumbency when being fed. The use of gastrostomy or jejunostomy tubes are considered preferable over oesophagostomy tubes in high risk patients (Hodshon and Tobias, 2014).
When administering blenderized food, tube blockages can be prevented by straining food prior to delivery and by avoiding the administration of solid oral medications, such as crushed tablets, via feeding tubes. Minor blockages can be managed by repeated flushing and suction with warm water or by instilling a small volume of carbonated soft drink in the tube.
Any resistance, coughing, gagging or signs of nausea during feeding should prompt immediate VS notification so the most appropriate action can be taken.
Dislodgement of a tube requires consultation with the VS to discuss removal and replacement.
Anorectic patients receiving enteral nutrition should be monitored closely for decreases in blood phosphate, magnesium and potassium levels, which could be indicative of the metabolic disorder, refeeding syndrome. Patients at risk of developing this condition must be carefully managed. Chan (2015) recommends gradual restoration of fluid balance and conservative estimation of energy requirement, with no more than 20% resting energy requirement (RER) provided on day 1, rising incrementally over 4 to 10 days.
Any dressing and bandage surrounding the exit site of a feeding tube should be removed and replaced on a daily basis to enable the stoma to be examined for signs of infection and patient discomfort (Michel, 2004; Firth, 2013).
Conclusion
This paper has provided a practical overview of the steps involved in placing commonly used feeding tubes. For further information regarding the underpinning evidence base, principles and nursing care associated with the use of this, and other, assisted feeding techniques, readers are advised to consult the list of references provided.
Key Points
It is the responsibility of veterinary surgeons and the veterinary nursing team to ensure the early identification of patients in need of nutritional support.
Collaboration between members of the veterinary healthcare team is essential to determine the most appropriate method and route of nutritional delivery, alongside the patient's nutrient needs and feeding goals.
A feeding method that utilises as much of the functioning gastrointestinal tract as possible should be adopted, while also ensuring its suitability for the patient's condition and initial hospitalisation period.