

Within human and veterinary surgery, pre-paring the surgical site for incision in-volves removing the maximum amount of organic matter, as well as transient and resident flora. This can be achieved through using correct scrubbing techniques (Bowers, 2012).
Historically, veterinary nurses have used the circular scrub technique, also known as ‘target’ or ‘bullseye’ (Swales and Cogan, 2017; Mann, 2018). This uses circular motions starting with the point of incision and working outwards, moving bacteria to the periphery (Mangram et al, 1999; Bowers, 2012). However, the back-and-forth technique has recently been adopted by some veterinary practices due to its popularity in human medicine (McMillan, 2014). The back-and-forth skin preparation technique starts at the incision site and works outwards to the periphery in an up and down motion (Roberts, 2013) and uses friction as well as pressure (Stonecypher, 2009), allowing the first five dermal layers of the skin to be penetrated where most bacteria reside (Stonecypher, 2009). With both techniques, the applicator is disposed of each time it completes a clean of the surgical site and repeated for either a set amount of time or until the applicator comes away clean (Swales and Cogan, 2017).
Research by Roberts (2013) and McMillan (2014) suggested however, that one technique may potentially be more effective than the other. Both papers suggested that the circular technique does not reach all of the cracks and fissures in the skin. This is further evidenced by Stonecypher (2009) who found that the back-and-forth technique may also be more effective due to the friction that is formed as well as the increased surface area coverage. The research aimed to determine if either technique was more effective than the other at removing bacterial contamination prior to surgery, and hence improve asepsis within veterinary surgery.
Literature review
The gold standard provision in veterinary care is to utilise evidence-based medicine to help evaluate the weight of evidence and guide clinical decision making which will ultimately increase animal welfare standards. When examining skin preparation techniques, we see a historical level of evidence informing decision making, and a reliance on tradition rather than evaluation. New ideas, concepts or techniques may emerge within other disciplines, some of which may be applicable and/or transferable within the veterinary domain.
Reviewing the literature, there is evidence to suggest that one skin preparation technique may be more beneficial than the other due to the back-and-forth technique which increases surface area and uses friction as well as pressure to help remove bacterial debris from the surgical site (Stonecypher, 2009). Shellim (2007) suggested that the mechanical action of scrubbing was also important, favouring the back-and-forth technique due to increased mechanical action of scrubbing utilised in this technique. Roberts (2013) further suggested that the circular technique used in the same direction does not allow some cracks and fissures of the skin to be fully disinfected, adding weight to the argument that this technique is superior in terms of asepsis. Because it is used predominantly with human surgery, this may also lead to the unsubstantiated assumption that the technique may be considered ‘superior’ to other techniques.
When performing a scrubbing technique, excessive force should be avoided as this encourages some bacteria to come to the skin surface, contaminating the surgical site (Roberts, 2013). Knowles (2009) investigated the efficacy of chlorhexidine gluconate and its use in practice, using the circular technique to prepare the surgical site. Their research suggested that rubbing the surgical site may just be as effective as scrubbing in reducing bacterial counts, indicating that the circular technique may be just as effective as back-and-forth technique due to a reduced scrubbing action. Excessive scrubbing can also cause skin irritation as well as causing resident flora from deep within the skin to rise to the surface (Baines, 1996; Roberts, 2013). Resident flora is bacteria which colonises the hair follicles and sebaceous glands (Roberts, 2013). Many veterinary practices use the circular technique as a matter of routine with many practices experiencing few asepsis problems using this method. Recent studies corroborate these findings suggesting that failure to achieve asepsis is due to bacterial resistance rather than skin preparation technique (Swales and Cogan, 2017; Mann, 2018).
Bowers (2012) stated that regardless of the pattern used, the area should be scrubbed until the swabs come away clean and for the recommended time as stated within the manufacturer's guidelines. This literature review concluded that regardless of the technique for skin preparation used within veterinary practice, as long as the skin is clean from organic matter and correctly disinfected according to the manufacturer's instructions, the choice of technique is irrelevant.
Finally, skin preparation techniques also need to be considered before pre-operative hair removal, an important factor both in the human and veterinary domain. Research by Mangram et al (1999), found that clipping human hair 24 hours prior to surgery increased the risk of a surgical site infection (SSI), most likely due to microscopic cuts in the skin leading to bacterial contamination. Extrapolating these results to the veterinary domain, pre-surgical preparation of the skin should be performed immediately prior to surgery in order to help reduce the risk of SSI.
Overall, there appears to be mixed opinions about which technique may be the most effective skin preparation prior to surgery in reducing bacterial load, and this may be because there are preferences within the human and veterinary fields historically rather than from evidence-based research. Within veterinary practice today, we should be moving towards evidenced-based research to aid our clinical decisions and improve patient care. This research aimed to determine if either technique was more effective at reducing the potential for SSI and help aid the veterinary professional in clinical decision making.
Methodology
Ethical consent was gained from the Askham Bryan College ethics board (NIC13051712). The participants were randomly selected to form two groups (five per group). No selection limitations or exclusions were placed in relation to breed, hair type or indoor/outdoor living status. One group underwent the circular scrub technique, the other group underwent the back-and-forth scrub technique. For each patient, prior to use, the clipper blades were thoroughly cleaned and disinfected. The surgical area was then clipped on the left flank using size 40 clipper blades, with the clippers held flat and close to the skin to prevent damage (Mangram et al, 1999; Bowers, 2012).
To prevent contamination, disposable gloves were worn throughout the scrubbing procedure and disposed of between patients. Non-lint gauze swabs were thoroughly soaked in the scrub solution (chlorhexidine gluconate diluted with purified water, 1:1 dilution) prior to use to allow maximum removal of dirt and grease (Baines et al, 2012), and the skin scrub was carried out for 3 minutes using a timer. When carrying out the circular technique, the scrubbing started at the incision site and worked outwards in a circular motion to the periphery (Roberts, 2013). When carrying out the back-and-forth method, the scrub began at the incision site and worked outwards to the periphery in an up and down motion (Roberts, 2013). Due to time constraints, a number of nurses were pre trained and completed the skin preparation and sampling prior to surgery.
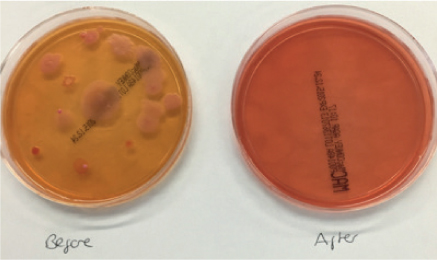
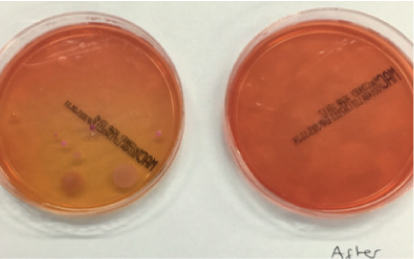
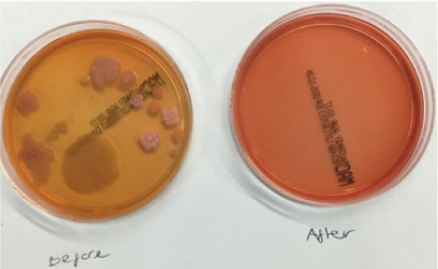
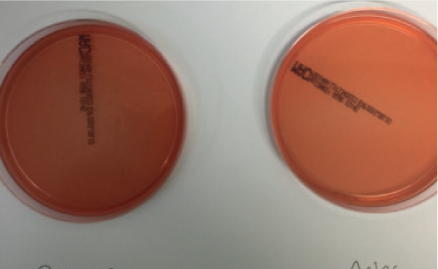
Using a plain sterile swab, a sample was taken from the incision site before and after scrubbing with the sample taken prior to scrubbing forming the control group, to allow a comparison to be made. The sample of bacteria was then placed onto a MacConkey agar plate using the quadrant-streak method (Box 1) and labelled with the patient's identification, the technique used, before or after scrub and the date. The agar plates were sealed and incubated at 38.5°C for 48 hours. The colonies were then counted and recorded as ‘colony forming units’ (CFUs) and each agar plate was also photographed.
All patients received a final scrub of chlorhexidine gluconate and surgical spirit (approximately 1 ml) immediately prior to surgery to ensure sterility and minimal levels of bacteria were present after the swabs had been taken (Association of Surgical Technologists (AST), 2008; International Cat Care, 2017).
Minitab was used to statistically analyse the quantitative data. All data were tested for normal distribution using the Anderson-Darling Test (circular scrub techniques before A2=0.31, p=0.352, circular scrub technique after A2=1.06, p=<0.005; back-and-forth technique before A2=0.48, p=0.120, back-and-forth technique after A2=1.20, p=<0.005). As the data were not normally distributed the researchers did not undergo checks for equal variance (Levene's test) and therefore non-parametric tests were selected. Wilcoxon signed rank test were performed on each patient's CFU count before and after scrub to identify any statistically significant difference. A Mann-Whitney U Test was performed to determine if there was any difference between the two scrub techniques to help identify if either technique was more effective than the other in reducing bacterial load prior to surgery.
Results
Table 1 shows the CFU counts ‘before’ and ‘after’ skin preparation when using the circular technique for a flank ovariohysterectomy. The data show three of the patients received 100% reduction in CFU's out of a sample size of five. Table 2 shows the CFU count for ‘before’ and ‘after’ skin preparation when using the back-and-forth technique for a flank ovariohystectomy (Figures 1–4). The data show that four out of five patients received a 100% reduction in CFU counts.
| Patient ID | CFU count before | CFU count after |
|---|---|---|
| 1 | 24 | 0 |
| 2 | 38 | 14 |
| 3 | 33 | 1 |
| 4 | 1 | 0 |
| 5 | 4 | 0 |
| Patient ID | CFU count before | CFU count after |
|---|---|---|
| 1 | 5 | 0 |
| 2 | 24 | 0 |
| 3 | 3 | 1 |
| 4 | 6 | 0 |
| 5 | 40 | 0 |
The data were statistically analysed using Minitab. As the data were not normally distributed, non-parametric tests were performed. Wilcoxon Signed Rank Tests were used to determine if there was any statistically significant difference in CFU counts for ‘before’ and ‘after’ for each technique. The results found that there was no statistically significant difference between the ‘before’ and ‘after’ CFU counts (circular scrub technique, Wilcoxon signed-ranks test: Wilcoxon statistic=0.0, N=5, p=0.059 (back-and-forth scrub technique, Wilcoxon signed-ranks test: Wilcoxon statistic=0.0, N=5, p=0.059).
A Mann-whitney U test was performed to determine if there was any difference between the two scrub techniques in reducing CFU counts. There results showed that there was no statistically significant difference in reducing CFU counts with either technique (Mann-Whitney U test: W=27.0, N=5, p=1.0000).
Discussion
Table 1 shows the data for the circular scrub method for five individual patients; in three of the patients there was 100% reduction in CFUs. Patient two showed 63% reduction of CFUs and patient three showed 96% reduction. As these patients demonstrated, 100% reduction in all patients was not achieved, and this could support the theory that the back-and-forth scrub technique may be more effective. However, patients two and three both had higher CFU counts compared with the other patients prior to surgery. This could further suggest that a longer scrub or pre-operative bathing 24 hours prior to surgery may be beneficial (Roberts, 2013).
Table 2 displays the data for the back-and-forth scrub technique for five individual patients. The data demonstrated that in this sample, 100% reduction in CFUs was achieved in four of the patients using this technique. Patient three had a 66.6% reduction of CFUs, but had a lower CFU count prior to skin preparation in comparison to the other patients. This could lead us to consider that the disinfection of the skin was not fully effective, possibly due to too much friction applied as discussed by Roberts (2013) whose research suggested that too much friction can cause residual flora to rise to the surface on the skin.
During data collection a problem was encountered regarding the incubation time for the agar plates. When incubating the first sample, it was checked as initially planned after 24 hours as suggested by Swales and Cogan (2017), however no CFUs had formed on the agar plate. The student veterinary nurse performing the data collection discussed the problem with the veterinary surgeon and it was agreed that the sample should be incubated for a further 24 hours. Following this, CFUs did form on the agar plate so a 48 hour incubation period was then initiated for all other samples. However this could have been avoided prior to commencing research, had a pilot study been conducted first.
A variable which may have affected the results was that due to time constraints, several people performed the scrub technique on different patients. The researchers addressed this by pre training all personnel performing the data collection process, however different pressures may have been applied when scrubbing, which may have caused bacteria deep within the skin to rise to the surface, as highlighted by (Knowles, 2009), therefore this may have influenced these results.
A review of skin disinfectant products has already been undertaken by Dumville et al (2013) which found that there was some evidence albeit weak, that pre-operative skin preparation using 0.5% chlorhexidine gluconate in methylated spirits reduced SSI more than the other preparations tested. This research used chlorhexidine gluconate diluted with purified water, dilution 1:1 but potential future research could duplicate this study and instead use chlorhexidine gluconate in methylated spirits as used by Dumville et al (2013) in reducing SSI.
Future studies should ensure one individual performs the scrub techniques for the entire sample to control the limitations to this study. Consideration should also be given to checking the disinfectant for bacterial resistance prior to use, assessing the living status (indoor versus outdoor feline) as well as sampling a larger population. Furthermore an interesting comparison study would be comparing flank versus midline incision (generally breed specific in felines) as potentially a midline incision has greater contact with objects or the ground such as soil that could carry a high bacterial load. Other recommendations include examining the pros and cons of pre-operative bathing prior to surgery. However, it is important to note that this may be contraindicated in those patients that are not contaminated as pre-operative bathing can cause increased hair shedding, exfoliation of the skin cells and growth of resident bacteria (Bowers, 2012). Finally further follow-up studies could explore using a pre-determined number of colonies of a non-pathogenic bacteria such as Lactobacillus, inoculated onto the skin. Using the scrub preparation techniques as a comparison, the potency of each technique could be compared by counting the reduction in CFUs from the known sample with samples taken after each scrub technique was performed, as this may also elucidate a clearer distinction between the two techniques.
This research was not able to conclude that either technique was better than the other at reducing bacterial counts, which is supported by the findings of Swales and Cogan (2017) and Mann (2018); however this may be due to the small sample size. In all of the patients prepared using either technique, there was a decrease in CFU count prior to surgery which therefore reduced the likelihood of that patient experiencing a SSI.
Conclusion
Veterinary nurses are at the forefront of increasing their knowledge using evidence-based practice to aid gold standard patient care. This research suggests that veterinary nurses can feel confident choosing to use either the circular technique or the back-and-forth technique to prepare the skin prior to surgery, and that this decision is based on science-led research rather than ‘tradition’. This study shows that despite the small sample size, in the case of flank ovariohysterectomy, either scrub technique is highly effective in reducing bacterial load prior to surgery, therefore reducing the risk of SSIs.