

Arterial blood pressure is a common parameter assessed in both conscious and anesthetised patients for numerous reasons. These include monitoring disorders, such as renal disease, cardiovascular disease and endocrine disease, and, most commonly, as a parameter to monitor the cardiovascular status of an animal under anaesthesia. Measuring blood pressure is a widely recognised element in patient care because both hypertension and hypotension can significantly affect the health of patients (Sturgess, 2016).
This article summarises both invasive and non-invasive blood pressure (NIBP) techniques available to measure arterial blood pressure in patients and discusses the causes of potential errors that may lead to inaccurate measurements. It describes the proper use of blood pressure measurement devices and interpretation of the measurements obtained from them.
Intravascular pressures
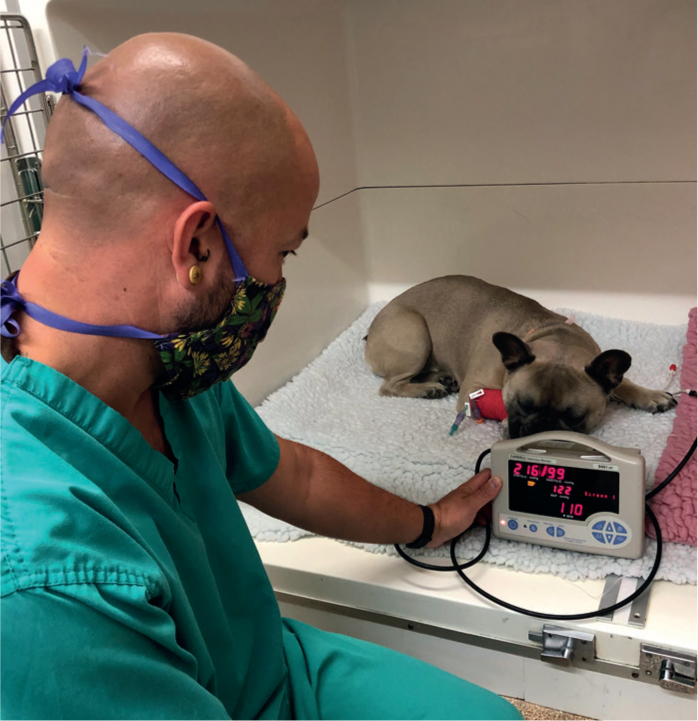
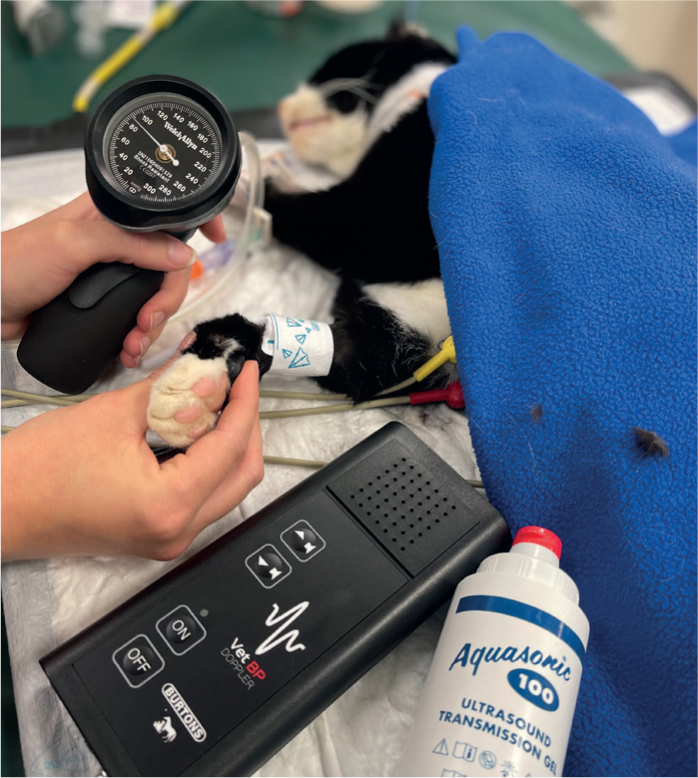
Blood pressure, or more accurately intravascular pressure, is the pressure that blood physically exerts on a vessel wall. This pressure is important because the difference in intravascular pressure at any two points in the vascular network is the driving force for blood circulation. The pressure found at the root of an aorta is much more than the vena cava pressure, ensuring blood will flow from the arterial side to the venous side, delivering nutrients and oxygen to cells located along this path. The most common intravascular pressure measured in small animals is the peripheral arterial blood pressure. This is most commonly measured indirectly via a surface-applied pressure cuff around a limb or tail base using flow detection methods such as oscillometry (Figure 1) or Doppler ultrasound (Figure 2) (Clarke et al, 2015; Haskins, 2015).
Intravascular pressures can also be measured in small animals directly. This has been shown to have much higher accuracy than indirect methods, and this also allows for continuous measurements to be read (Cooper and Cooper 2012; Cooper 2015; Waddell and Brown, 2015) (Figures 3 and 4).
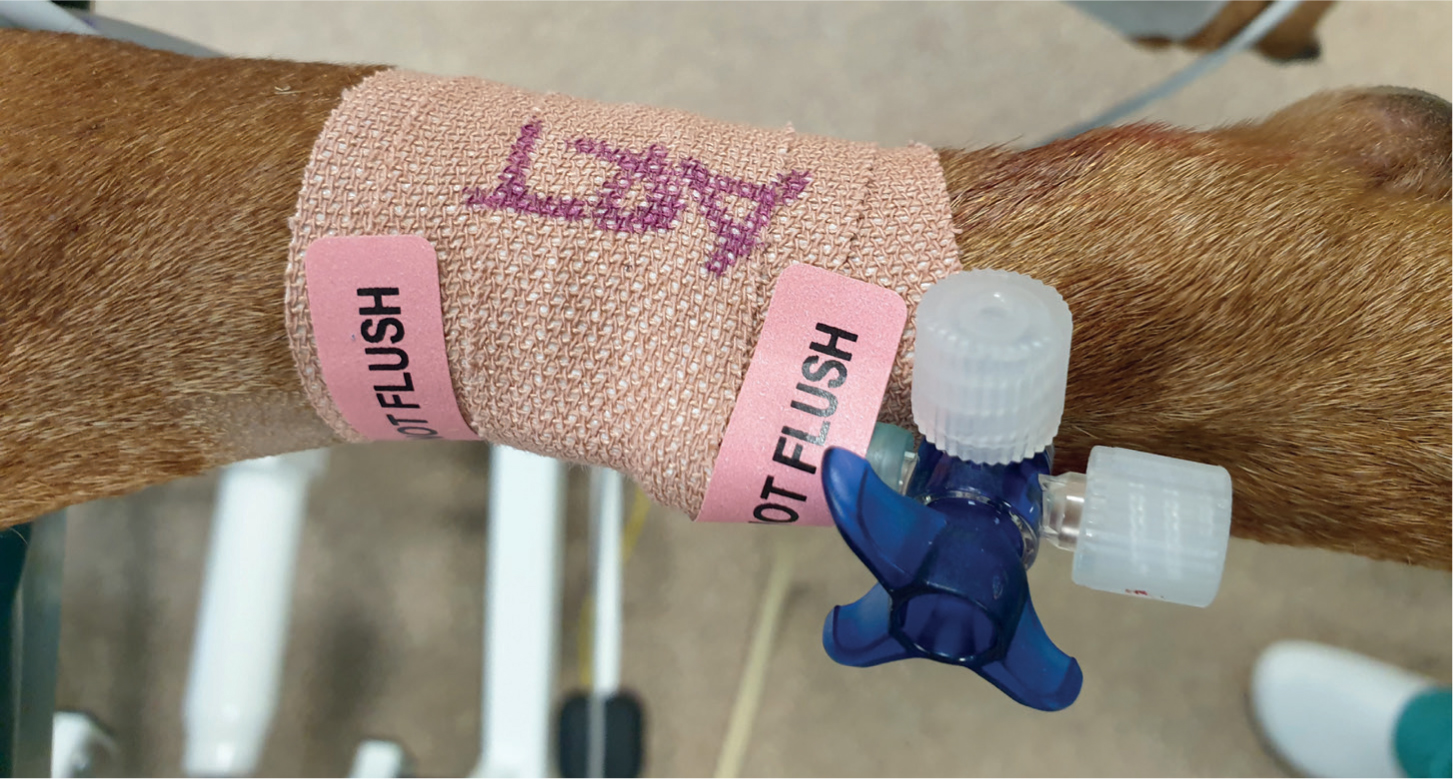
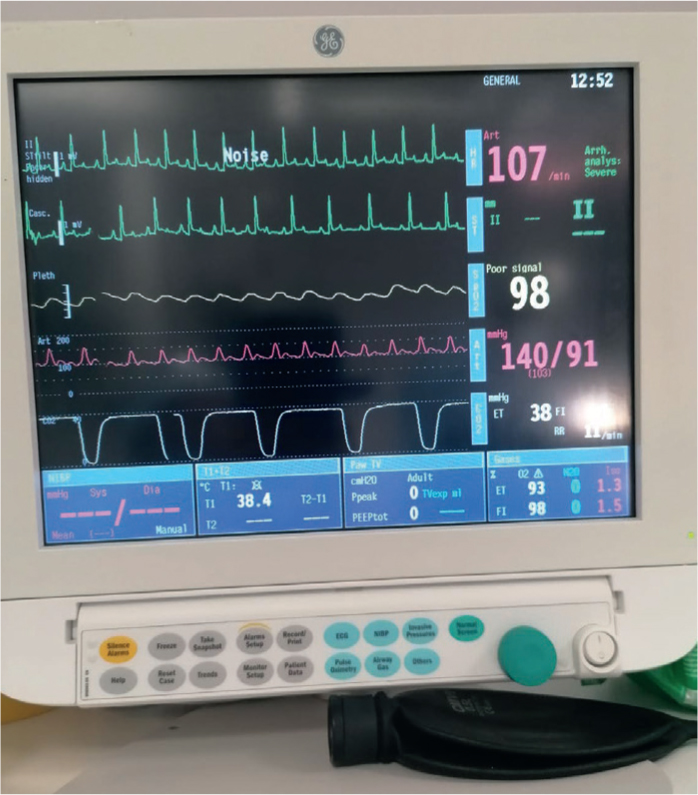
An arterial catheter is placed into a peripheral artery, by an experienced veterinary nurse or surgeon, most commonly the dorsal metatarsal or femoral artery. This catheter is attached to a monitor which provides ‘real time’ information, such as systolic (SAP), mean (MAP) and diastolic arterial pressure (DAP), heart rate and provides a waveform. Because of this, direct monitoring is considered the best technique to monitor blood pressure.
This method of measurement is especially valuable when monitoring critically ill patients to detect rapid blood pressure changes. Despite its obvious advantages, direct blood pressure monitoring is not performed as much as indirect because of the higher costs, the need for specialised equipment and the increased skills needed to place and then maintain the arterial line. Arterial blood pressure measured this way is typically reserved for use in perioperative and intensive care veterinary medicine. More active patients rarely tolerate catheter placement and will be at increased risk of the catheter becoming dislodged because of movement.
General measurement principles
One of the most popular NIBP methods is Doppler ultrasound blood pressure monitoring. This technique involves a Doppler probe with a pair of piezoelectric crystals inside being placed on the skin in an area over a peripheral artery. A pressure cuff is applied circumferentially to the tail or limb of the patient, and the probe placed distally to the cuff (Figure 5). Blood flowing through an artery will produce an audible sound in the Doppler machine. The cuff is inflated until no sound is audible and then deflated slowly until sound returns. This enables systolic pressure to be determined.

This technique is not suitable for dogs or cats as a means of determining DAP or MAP.
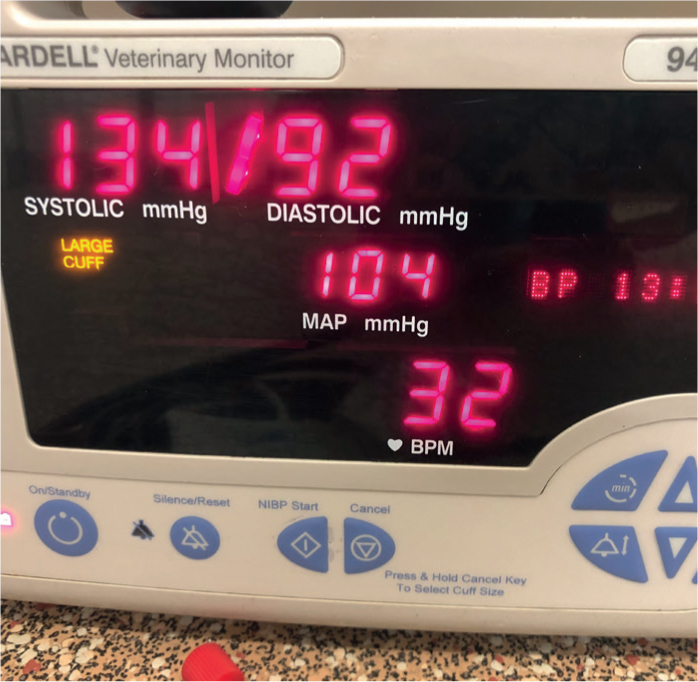
The Doppler technique requires more skill and more time than the oscillometric technique, which is another option. Oscillometry means that a pressure cuff is connected to a device, which detects oscillations in the arterial wall during blood flow while the cuff is deflating. An oscillometric machine usually displays the pulse rate along with MAP, DAP and SAP. (Figure 6). It is sometimes difficult to obtain an accurate reading with the oscillometric technique if the patient has significant bradycardia or tachycardia, cardiac arrhythmias, vasoconstriction, or when the patient cannot be kept still (Savino and Sierra, 2018; Thomas and Boller, 2018). Oscillometric blood pressure monitoring is particularly useful as it requires less technical skill to operate than the Doppler method, can be programmed to measure blood pressure at timed intervals and requires less patient handling.
Patient position and limb selection
An incorrect patient position or limb selection can result in an inaccurate reading. Whichever position is most comfortable for the patient is usually the best position. Laterally recumbent and lying immobile and relaxed is usually the best choice (Rondeau et al, 2013).
The cuff can be placed on the forelimbs or hindlimbs with the areas close to the tarsus or carpus being effective, or the tail (Figure 7). The tail is an option for breeds with dyschondroplasia such as Basset Hounds and Dachshunds, where placement on the forelimbs or hindlimbs may prove difficult. Cuff placement where the patient tolerates it best is highly recommended.

To obtain the most accurate blood pressure measurements, the cuff should be as close to the level of the right atrium as possible (Waddell and Brown, 2015).
Cuff size and placement
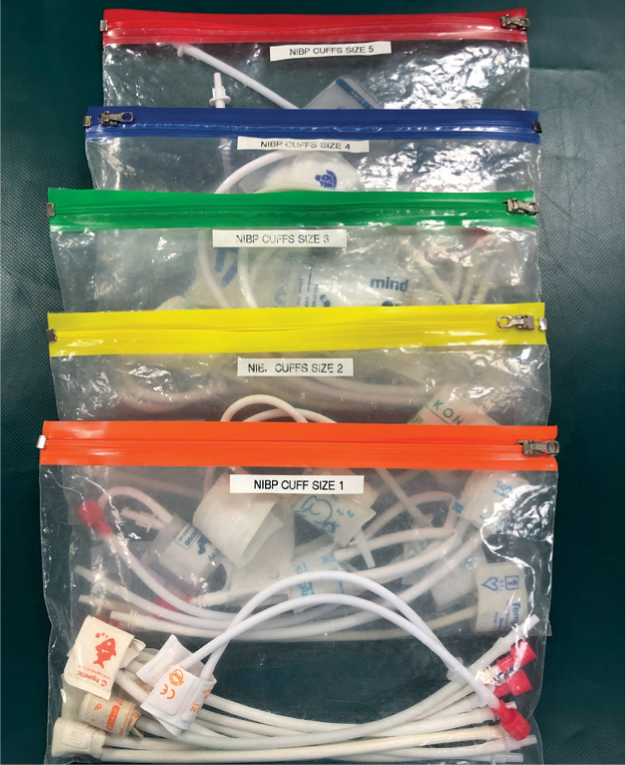
It is critical to use the correct cuff size for an accurate blood pressure measurement. If the cuff is too narrow this can give falsely high readings. If it is too wide it can result in erratic readings that underestimate the blood pressure (Schauvliege, 2016). Use the limb or tail circumference where the blood pressure is being measured to determine correct cuff size. Cuff width needs to be 30–40% of the circumference of the site where it is being applied (fore-limb, hindlimb or tail) (Acierno et al, 2018) (Figure 8).

However, if the measurement falls between two cuff sizes, choose the wider of the pair. Poor cuff selection and placement are the most common cause of blood pressure reading errors (Bryant, 2010).
Line up the cuff bladder with the artery and place it directly over. There is an artery arrow imprint on some cuffs (Figure 9). This does not mean the arrow points in the direction of blood flow. It means the arrow must overlie the anatomic vessel site in the limb or tail. Direct the tubing towards the monitoring equipment and away from the animal.

Take care to make sure the cuff is placed close to the extremity without being too tight, since this can slow blood flow resulting in an erroneously low blood pressure reading. Take this into consideration when securing the cuff using medical tape.
Doppler ultrasonic blood pressure measurement
Doppler ultrasonic blood pressure measurement requires:
- Ultrasonic conductance gel
- Small, quiet clippers equipped with clean blade
- Sphygmomanometer
- Correct size pressure cuff
- Plugged in or fully charged Doppler ultrasound machine
- Headphones for Doppler ultrasound machine (optional, but recommended)
- Assistant (if needed).
Procedure
To carry out Doppler ultrasonic blood pressure measurement:
- Gather the required supplies.
- Position the patient in a relaxed lateral recumbence while holding the limb or tail at the approximate level of the right atrium.
- Clip the hair away from the area over the artery if the patient tolerates this with quiet, gentle clippers. Alternatively to ensure there is excellent contact between the Doppler probe and the skin to detect blood flow in the artery, use alcohol to dampen the hair and skin and apply ultrasound coupling gel. It is not necessary for the probe to have direct contact with the skin. The probe needs a layer of gel as an interface.
- After securing a deflated cuff over the artery, attach the sphygmomanometer. Secure the cuff mid radius when using the forelimbs to measure blood pressure. Secure the cuff next to the hock when using the hindlimbs. Medical adhesive tape might be needed to effectively secure the cuff.
- Apply ultrasonic gel to the Doppler probe's surface.
- Lie the gel-covered probe on the clipped skin over the artery. Common locations include the dorsal pedal artery, digital artery, and coccygeal artery.
- Use fine movements to adjust the probe until you hear the arterial rhythmic ‘whooshing’ sound.
- Inflate the sphygmomanometer to between 30 and 40 mmHg beyond the point where the arterial sounds are no longer audible.
- Deflate the cuff slowly until the sounds are audible again. This marks the systolic blood pressure.
- Let the cuff deflate fully so blood flow returns to the limb.
- Discard the first measurement and repeat the procedure between 3 and 7 times and then calculate the average of these readings to get the results.
- Record the average SAP as well as cuff size, cuff location and results in the patient record.
Standard oscillometric sphygmomanometry blood pressure measurement
Oscillometric sphygmomanometry blood pressure measurement requires:
- Oscillometer with power cord
- Correct size pressure cuff
- Assistant (if needed).
Procedure
To carry out standard oscillometric blood pressure measurement:
- Gather the required supplies.
- Position the patient in a relaxed lateral recumbence while holding the limb or tail at the approximate level of the right atrium.
- Position the cuff on the limb or tail. The cuff bladder (the part which fills with air) must be centred over the palpable pulse if this is possible.
- Measure for and place the cuff above the carpus in cats or small dogs.
- Measure for and place the cuff above the metatarsal in large dogs.
- Push the button on the oscillometer which starts pressure readings. Discard the first measurement and repeat the procedure between 3 and 7 times, and then calculate the average of these readings to get the results.
- Record the average DAP, SAP and MAP, as well as cuff size, cuff location and results in the patient record.
Conclusion
It is important to properly educate nurses who will perform blood pressure measurement and keep them updated on the correct use of equipment and procedures. It is necessary to repeat results to achieve standardisation of the measuring technique. In critical patients where accuracy is vital, direct monitoring is still the best way to measure blood pressure with the highest level of accuracy.
Terms definitions
- Blood pressure — blood pressure measured along the main artery walls
- Diastolic blood pressure — the level the arterial blood pressure falls to during ventricular diastole, or relaxation
- Systolic blood pressure — peak arterial blood pressure following ventricular systole, or contraction
- Hypotension — low blood pressure
- Hypertension — high blood pressure
Tip:
A small, clear organiser or file folder is useful to keep cuffs separate, easily accessible and neatly organised.
KEY POINTS
- The ‘gold standard’ of measuring blood pressure is direct monitoring.
- Standardising the measurement process when measuring indirectly will produce the most accurate results.
- Interpret results of indirect measuring with care taking other parameters into account as well as possible inaccuracy causes.